Clinical Summary
A 55-year-old woman presents with a unilateral solid ovarian mass measuring 7.5 cm in greatest dimension. An oophorectomy is performed and shows a circumscribed mass with white, firm cut surfaces.
Master List of Diagnoses
- Benign Brenner tumor
- Carcinoid
- Fibroma
- Malignant Brenner tumor
- Metastatic urothelial carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 31, and is benign Brenner tumor in the ovary. The information provided in this case was accurate and correct at the time of publication in 2020. Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
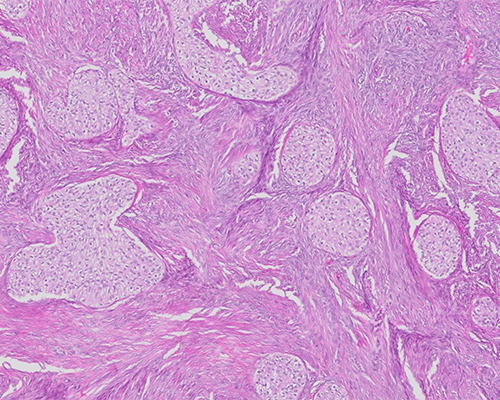
Histologic sections show small nests of cytologically bland epithelial cells with abundant clear to eosinophilic cytoplasm distributed within a fibromatous stroma. The nuclei are small and slightly irregular, with small nucleoli. There is no significant cytologic atypia or mitotic activity. Occasional nests have small cyst formation in the center. The findings are consistent with a benign Brenner tumor.
Similar to other epithelial ovarian tumors, Benner tumors are classified as benign, borderline/atypical proliferative, or malignant. Benign Brenner tumors account for approximately 5% of all benign ovarian epithelial tumors and are typically found incidentally in women in the 5th to 7th decades of life. Brenner tumors are commonly associated with other ovarian neoplasms, including mucinous-type tumors.
Grossly, benign Brenner tumors are small (typically less than 2 cm) and unilateral. Fewer than 10% of cases occur bilaterally. These tumors are solid, firm, and well-circumscribed, with variable stromal calcifications. Small cysts are often present, but benign Brenner tumors are rarely predominantly cystic.
Microscopically, the tumors are composed of solid to cystic nests of epithelial cells embedded in a fibrous stroma. The epithelial cells have a urothelial cell-like appearance, with abundant clear to pale eosinophilic cytoplasm and small nucleoli. Nuclear longitudinal grooves are common. There is no cytologic atypia, and mitoses are rarely present. Mucinous epithelium may be seen and is often associated with cystic dilation of nests. The background fibrous stroma frequently contains coarse calcifications. By immunohistochemistry, benign Brenner tumors are positive for CK7, p63, GATA3, uroplakin III, and thrombomodulin. CK20 is typically negative but may be focally positive. The majority of tumors are negative for WT1. No recurring molecular abnormalities have been identified in Brenner tumors.
Borderline/atypical proliferative Brenner tumors are often larger than benign Brenner tumors, with an average diameter of 18 cm. Clinical behavior is typically benign, although rare local recurrences occur. These tumors are predominantly cystic but may contain variable solid areas, often representing a coexisting benign Brenner component. Cysts often show papillary or polypoid projections into the cyst lumens. Histologically, these tumors resemble non-invasive, low-grade urothelial neoplasms. Nests are large and crowded and may show fusion, as a result of epithelial proliferation that exceeds what is seen in benign Brenner tumor. Nests often show cystic cavitation, and mucinous epithelium is common. Cytologic atypia and mitotic activity are present, but there is no stromal invasion. A benign Brenner tumor component is often present in the background.
Malignant Brenner tumors are uncommon ovarian carcinomas and represent less than 5% of all Brenner tumors. They are unilateral and large (averaging 16 - 20 cm in dimension) with variable solid and cystic components. Most tumors are confined to the ovary at diagnosis, and malignant Brenner tumors have a better prognosis than other epithelial ovarian carcinomas. Histologically, malignant Brenner tumors are associated with a benign or borderline/atypical proliferative Brenner tumor component. They are composed of irregular nests of malignant cells with stromal invasion, often associated with a desmoplastic reaction. The cells are hyperchromatic, with pleomorphic nuclei and frequent mitotic figures. Mucinous and squamous differentiation is common.
Carcinoid, or well-differentiated neuroendocrine tumor, of the ovary is uncommon but may occur as a monodermal teratoma or a somatic-type malignancy arising from a teratoma or dermoid cyst. Mean age at diagnosis is in the early 6th decade, and most tumors are unilateral. Carcinoids demonstrate a variety of histologic patterns. Cells have round nuclei with stippled (“salt and pepper”) chromatin and pale eosinophilic cytoplasm. The background stroma may be prominent and is often fibromatous. Immunohistochemistry shows positivity for synaptophysin and chromogranin. CK7 and CK20 show variable positivity depending on the histologic pattern.
Fibroma is the most common pure ovarian stromal tumor and represents approximately 5% of all ovarian tumors. Most tumors are unilateral and occur at an average age of 50 years. Fibromas are common in patients with nevoid basal cell carcinoma syndrome (Gorlin syndrome). Tumors associated with this syndrome tend to be bilateral and occur in younger patients. Approximately 1% of patients develop concurrent ascites and pleural effusion (Meigs syndrome). Fibromas are characterized by intersecting fascicles of spindled to ovoid cells with bland nuclei and scant cytoplasm. Coarse calcifications may be present. The tumors are immunoreactive for inhibin and calretinin.
Metastatic urothelial carcinoma involving the ovaries is uncommon. Invasive urothelial carcinoma is composed of malignant cells arranged in diffuse sheets or infiltrating nests, cords, or single cells. There is nuclear pleomorphism, and mitotic activity is increased. Malignant cells are positive for CK7, CK20, p63, thrombomodulin, and GATA3. Many tumors are also positive for uroplakin III. Differentiating metastatic urothelial carcinoma from malignant Brenner tumor can be challenging, but in the latter, background typical Brenner lesions are likely to be present, while metastatic urothelial carcinoma is often associated with a known extra-ovarian primary.
Supplementary Questions
- Which of the following statements is most accurate regarding benign Brenner tumors?
- Approximately 90% of patients present with bilateral ovarian masses.
- Diagnosis can be confirmed by identifying a characteristic recurring molecular alteration.
- The classic gross appearance is multicystic, with minimal intervening solid components.
- They are positive for CK7 and p63.
- Tumors are composed of large infiltrative nests composed of hyperchromatic cells with prominent nucleoli and frequent mitotic figures.
- Which of the following features is most supportive of a diagnosis of borderline/atypical proliferative Brenner tumor?
- Immunoreactivity for neuroendocrine markers
- Large, crowded nests of cells
- No cytologic atypia
- No mitotic activity
- Stromal invasion associated with a desmoplastic reaction
- Which of the following statements is most accurate regarding fibromas?
- Calcifications are not seen in these tumors.
- Fibromas are negative for inhibin and calretinin.
- Fibromas associated with Gorlin syndrome often occur in young patients.
- Most fibromas present with ascites and pleural effusions.
- The majority of fibromas present as bilateral ovarian masses.
References
- Amin MB. Histological variants of urothelial carcinoma: diagnostic, therapeutic and prognostic implications. Mod Pathol. 2009;22:S96-S118.
- Cuatrecasas M, Catasus L, Palacios J, Prat J. Transitional Cell Tumors of the Ovary: A Comparative Clinicopathologic, Immunohistochemical, and Molecular Genetic Analysis of Brenner Tumors and Transitional Cell Carcinomas. Am J Surg Pathol. 2009;33(4):556-567.
- Han G, Soslow RA. Nonserous ovarian epithelial tumors. Surg Pathol Clin. 2011;4(1):397-459.
- Kondi-Pafiti A, Kairi-Vassilatou E, Iavazzo C, et al. Clinicopathological features and immunoprofile of 30 cases of Brenner ovarian tumors. Arch Gynecol Obstet. 2012:285(6):1699-1702.
- Kurman RJ, Carcangiu ML, Herrington CS, Young RH, (Eds). WHO Classification of Tumours of Female Reproductive Organs. IARC Press, Lyon, France 2014.
- Logani S, Oliva E, Amin MB, et al. Immunoprofile of ovarian tumors with putative transitional cell (urothelial) differentiation using novel urothelial markers: histogenetic and diagnostic implications. Am J Surg Pathol. 2003;27(11):1434-1441.
Answer Key
- They are positive for CK7 and p63. (d)
- Large, crowded nests of cells (b)
- Fibromas associated with Gorlin syndrome often occur in young patients. (c)

