Clinical Summary
A 74-year-old woman with no prior history of cancer presents with a large abdominal mass. A large left adnexal mass is identified on a pelvic ultrasound exam. She undergoes a left salpingo-oophorectomy. Gross examination reveals an ovary weighing 795 grams and measuring 17 cm in the largest dimension. The outer surface appears unremarkable. Sectioning reveals the ovary is replaced by a solid mass that is negative for inhibin and CK20.
Master List of Diagnoses
- Atypical endometriosis
- Endometrioid ovarian adenocarcinoma
- Metastatic colonic adenocarcinoma
- Mucinous adenocarcinoma
- Sertoli–Leydig cell tumor
- Yolk sac tumor
Archive Case and Diagnosis
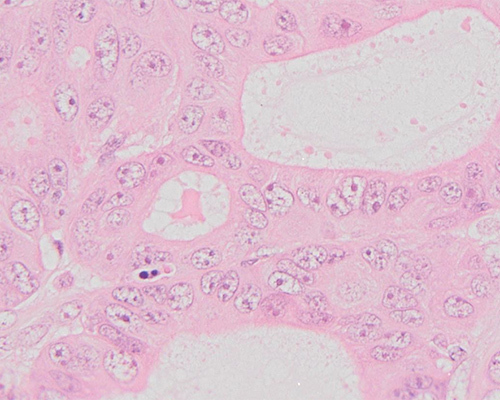
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 13, and is endometrioid ovarian adenocarcinoma (ovary). The information provided in this case was accurate and correct at the time of publication in 2020. Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
Sections show haphazardly arranged individual glands as well as areas of confluent, fused glands with a cribriform growth pattern. Tumor foci do not appear on the surface of the ovary but rather replace the ovarian stroma. Focally, there are also areas of solid growth of tumor cells. Tumor cells are cuboidal with round to oval nuclei with vesicular chromatin and apparent nucleoli. Typical features of an ovarian primary neoplasm are not identified in this case, such as squamous morules or differentiation, a papillary growth pattern, mucin, and psammoma bodies. Considering all these findings, this tumor is best diagnosed as endometrioid ovarian adenocarcinoma (EOA). These are graded the same as endometrial adenocarcinoma using the FIGO system, which is based on percentage of solid growth of glandular cells (not including areas of solid squamous growth) and appearance of nuclei. Less than 5% solid growth is considered grade 1, 5% - 50% is considered grade 2, and greater than 50% is considered grade 3. The presence of high-grade nuclear features (marked pleomorphism and prominent nucleoli) calls for the grade to be increased by 1 for tumors with grade 1 or grade 2 glandular growth patterns. Considering the FIGO grading criteria, this tumor is considered grade 2.
Endometrioid ovarian tumors (including benign, borderline, and malignant tumors) make up about 3% of all ovarian tumors, and EOA) make up about 15% of all ovarian carcinomas. EOA are usually found in women of older reproductive age or who are postmenopausal. One of the well-established precursors in the pathogenesis of endometrioid (and clear cell) ovarian adenocarcinoma is atypical endometriosis. In about 40% of EOA, atypical endometriosis is present concurrently. Fifteen to 20% of the time, there is an associated endometrial adenocarcinoma, which sometimes causes difficulty in determining the site of origin and whether these are synchronous or metachronous primaries. Similar to other ovarian carcinomas, CA-125 is usually elevated. Although increased body mass index is associated with endometrial carcinoma, this is not necessarily the case with EOA.
Lynch syndrome is the most important genetic association with EOA. Therefore, additional testing in this case should include microsatellite instability testing via either immunohistochemistry or polymerase chain reaction (PCR). Other genetic mutations involve ARID1A, PIK3CA, PTEN, and PPP2R1A. These are also associated with clear cell ovarian adenocarcinoma. CTNNB1 (which encodes beta-catenin) is another mutation found in EOA, but this is not associated with clear cell ovarian adenocarcinoma. One study found that 17% of EOA showed KRAS mutations.
The differential diagnosis includes atypical endometriosis and other surface-epithelial ovarian tumors such as serous or mucinous adenocarcinoma. Solid growth pattern and cytologic atypia, along with lack of surrounding endometrial-type stroma or hemorrhage, helps exclude atypical endometriosis. Lack of a papillary growth pattern and psammoma bodies helps to confidently exclude serous adenocarcinoma (although endometrioid adenocarcinomas with a papillary growth pattern do exist). The lack of mucin and mucinous cells helps exclude mucinous adenocarcinoma (although mucin-poor mucinous adenocarcinomas also exist).
Histologically, metastatic colon adenocarcinoma (MCA) typically shows mucin and dirty necrosis. In challenging cases, immunohistochemistry is useful with the following immunoprofiles:
- EOA: cytokeratin 7 (+), cytokeratin 20 (-), CDX2 (-)
- MCA: cytokeratin 7 (-), cytokeratin 20 (+), CDX2 (+)
Sex cord–stromal tumors such as Sertoli–Leydig cell tumors (SLCT) enter into the histologic differential diagnosis when there is a prominent trabecular growth pattern; hollow tubules that are round, small and/or cystic (so called “pseudoendometrioid”); eosinophilia of tumor cells and monomorphic round nuclei of tumor cells. Tumor cells in SLCTs are positive for inhibin and calretinin and negative for epithelial membrane antigen (EMA) and cytokeratin 7. The opposite immunoprofile is found in EOA.
- EOA: cytokeratin 7 (+), EMA (+), inhibin (-), calretinin (-)
- SLCT: cytokeratin 7 (-), EMA (-), inhibin (+), calretinin (+)
Yolk sac tumors (YST) have numerous histologic patterns, including endometrioid, and must also be included in the histologic differential diagnosis. In this case, the age of the patient is helpful, as YST are usually found in younger patients. The differential diagnosis can be challenging because EOA can show a focal component of YST. YST typically show other characteristic patterns that may help make this diagnosis. YST are positive for alpha-fetoprotein (AFP) and negative for EMA and cytokeratin 7. The opposite is true for EOA. Finally, one should be aware of the rare possibility of mixed tumors with components of both EOA and YST.
Supplementary Questions
- Which gene is considered characteristically mutated in endometrioid ovarian carcinomas but not in clear cell ovarian carcinomas?
- ARID1A
- CTNNB1
- PIK3CA
- PPP2R1A
- PTEN
- Which of the following immunoprofiles most favors the diagnosis of endometrioid ovarian adenocarcinoma?
- AFP negative, CK7 positive, inhibin negative
- CK7 negative, CK20 negative, inhibin negative, CDX2 negative
- CK7 negative, CK20 negative, inhibin positive, CDX2 negative
- CK7 negative, inhibin positive, calretinin positive
- MLH1 negative, MSH2 negative, inhibin negative, CK20 positive
- Which of the following is true regarding the clinical, histologic, and genetic features of endometrioid ovarian adenocarcinoma?
- Atypical endometriosis is seen in 40% of cases.
- Clear cell and endometrioid adenocarcinomas do not share the same genetic mutations.
- Concurrent endometrial carcinoma is found in 50% of cases.
- The absence of mucin is very helpful and completely excludes mucinous ovarian carcinoma and metastatic colonic adenocarcinoma.
- While only 3% of ovarian tumors are surface-epithelial derived, endometrioid ovarian adenocarcinomas account for 60% of all surface-epithelial ovarian tumors.
References
- Clement PB, Stall J, Young RH, eds. Atlas of Gynecologic Surgical Pathology. 2nd Ed. Philadelphia, PA: Saunders Elsevier. 2008;333-340.
- Ilenkovan N, Gourley C. Pathogenesis, Genetics, and Genomics of Non-High Grade Serous Ovarian Cancers. Hematol Oncol Clin N Am. 2018;32(6):929-942.
- Sookram J, Levin, B, Barroeta J, Kenley K, Pallav M, Krill LS. A case of ovarian endometrioid adenocarcinoma with yolk sac differentiation and Lynch Syndrome. Gynecol Oncol Rep. 2019;27:60-64.
- Young RH. Ovarian sex cord-stromal tumours and their mimics. Pathology 2018;50(1):5-15.
Answer Key
- CTNNB1 (b)
- AFP negative, CK7 positive, inhibin negative (a)
- Atypical endometriosis is seen in 40% of cases. (a)

