Clinical Summary
A 65-year-old man presents with vague abdominal pain. A computed tomography scan reveals an abdominal mass near the greater curvature of the stomach. Gross examination of the surgical resection reveals an ulceration of the mucosa and a corresponding predominantly submucosal 9 cm mass that is circumscribed, intramural, fleshy, and firm. There are areas of intratumoral hemorrhage.
Master List of Diagnoses
- Abdominal fibromatosis
- Gastrointestinal stromal tumor
- Leiomyosarcoma
- Sclerosing mesenteritis
- Solitary fibrous tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 29, and is gastrointestinal stromal tumor in the stomach.
Criteria for Diagnosis and Comments
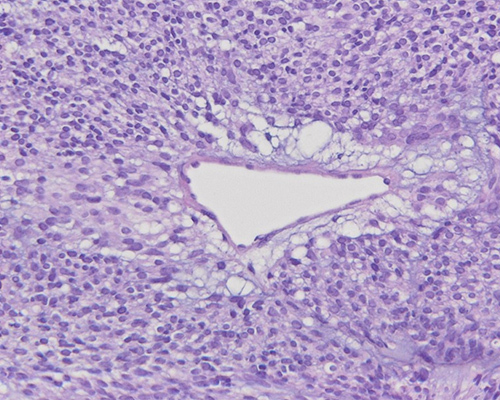
The histological sections demonstrate a circumscribed lesion comprised of spindled cells. The cells are arranged in fascicles and have a whorled appearance. Cell borders are not well-defined, and the cytoplasm is pale and fibrillary. The nuclei are oval with fine nuclear chromatin. Mild nuclear enlargement and atypia can be noted. Mitotic activity ranges from 6 to 20 mitotic figures per 5mm2. Occasional clusters of brightly eosinophilic wool-like fibers (skeinoid fibers) are present. Foci of hemorrhage and intratumoral necrosis are noted throughout the tumor. These features are those of a gastrointestinal stromal tumor (GIST), spindle cell type.
GIST is a mesenchymal tumor with no sex predilection commonly seen in the sixth decade. GIST rarely occur in children but, when present, are frequently associated with a genetic syndrome. Most GIST (60%-70%) arise in the stomach, 20% - 30% are seen in the small intestine, and the remaining 5%-10% occur in the esophagus, colorectum, omentum, and peritoneum. These tumors can be small and asymptomatic or large and bulky, presenting with obstructive symptoms. They can be single or multiple.
Morphologically, GIST are divided into three categories; spindle cell type (70%), epithelioid cell type (20%), or mixed type (10%). Spindle cell GIST display uniform spindle cells with pale eosinophilic, indistinct cytoplasm, oval nuclei, and paranuclear vacuoles. The spindle cells are arranged in fascicular, whorled, or storiform patterns. Palisading is a frequent feature, and eosinophilic structures known as skeinoid fibers are common. Spindle cell GIST more commonly arise in the stomach and small intestine. Myxoid change and osseous metaplasia are not uncommon. Epitheliod GIST are comprised of round to polygonal cells with round to oval nuclei. The cells are less cohesive and are arranged in sheets or nests. Mixed tumors are less common and have features of both epitheliod and spindle cells variants. Cystic degeneration, hemorrhage, and necrosis have been noted in all three types of GIST.
Immunohistochemically, a majority of GIST will label with CD117/c-Kit, primarily caused by activating mutations in the KIT or platelet derived growth factor A (PDGFRA) genes. Most KIT mutations involve exon 11 or exon 9. CD34 positivity is expressed in 80%-95% of tumors. DOG1 is a specific immunohistochemical marker; DOG1 and CD117/c-Kit positivity confirm the GIST diagnosis. In KIT/PDGFRA wild-type (WT) GIST, immunohistochemistry for succinate dehydrogenase subunit B protein may be done, showing aberrant loss of staining for this protein. Smooth muscle actin labeling has been noted in 30%-40% of GIST. S100 protein, desmin, and keratin can rarely be positive.
Up to 5% of GIST are immunohistochemically negative for c-Kit. These tumors are more common in the stomach, omentum, and peritoneum and have an epithelioid or mixed phenotype. They will either be KIT WT or will harbor PDGFRA mutations. BRAF V600E mutations have been noted in CKIT and PDGFRA WT GIST. The majority of GIST arise sporadically; however, 5% have been associated with genetic syndromes like Carney triad, neurofibromatosis type 1, familial GIST syndrome, and Carney–Stratakis syndrome.
A subset of syndromic GIST are associated with germline mutations in the succinate dehydrogenase complex (SDH). These tumors are more common in the stomach and are often epithelioid type, hypercellular with a plexiform or multinodular growth pattern. These SDH-deficient GIST are associated with Carney–Stratakis syndrome, Carney triad, pediatric GIST, or pediatric-type GIST in adults; they should not undergo risk stratification.
GIST risk stratification is based on mitotic rate, size, and location. The Armed Forces Institute of Pathology (AFIP) criteria divides risk by location within the gastrointestinal tract, the size of the tumor and the number of mitosis per 5mm2; it is outlined in the table below.
RISK STRATIFICATION OF PRIMARY GIST | |||||
Tumor parameters | Risk of progressive disease (%) | ||||
Mitotic index (per 5mm2) | Size | Gastric | Duodenum | Jejunum/Ileum | Rectum |
<5 | <2 cm | None | None | None | None |
<5 | >2 cm to <5 cm | Very low | Low | Low | Low |
<5 | >5 cm to <10 cm | Low | Moderate | Data is insufficient | Data is insufficient |
<5 | >10 cm | Moderate | High | High | High |
>5 | <2 cm | None | High | Data is insufficient | High |
>5 | >2 cm to <5 cm | Moderate | High | High | High |
>5 | >5 cm to <10 cm | High | High | Data is insufficient | Data is insufficient |
>5 | >10 cm | High | High | High | High |
For localized GIST, complete surgical resection is the first line of treatment. The tyrosine inhibitors targeting KIT and PDGFRA, imatinib and sunitinib malate, have been approved by the United States Food and Drug Administration for targeted GIST therapy. In fact, GIST with exon 11 KIT mutations have demonstrated the most dramatic response to imatinib therapy. GIST with PDGFRAA D842V mutations are resistant to imatinib. GIST can develop drug resistance to imatinib therapy; in such instances, sunitinib therapy is approved as a second-line agent. These therapies are approved for use as adjuvant and/or palliative modalities.
The rare entity formerly known as gastrointestinal autonomic nerve tumor (GANT) is now classified as GIST. The small bowel is the most frequently affected site followed by the stomach. Histologically, GANTs share the spindle and epitheliod cytomorphology typical of GIST. The distinguishing features of GANT are the presence of dendritic processes with dense neuroendocrine granules on ultrastructural examination.
Abdominal fibromatosis, also known as desmoid tumor, is a subset of infiltrative and locally aggressive clonal fibroblastic proliferations more frequently encountered in women than men (2:1) and in young adults (25-35 years). Most desmoid tumors occur sporadically, but they can be associated with familial adenomatous polyposis (FAP). On gross examination, these tumors are firm with a white cut surface and infiltrative borders. They are comprised of cytologically bland fibroblasts and myofibroblasts. The nuclei have open chromatin with a prominent nucleolus. The stroma can be dense and collagenous to myxoid. Delicate curvilinear, non-branching vessels are present. Necrosis and cystic degeneration are not present. 90% of desmoid tumors demonstrate nuclear beta-catenin labeling. In contrast to GIST, desmoids do not label with DOG1 and CD34; c-Kit/CD117 labeling is variable and often weak when positive.
Leiomyosarcomas are malignant smooth muscle tumors that can arise in the deep soft tissues, retroperitoneum, omentum, and mesentery of the gastrointestinal tract. In the stomach, they arise from the muscularis propria. Histologically, they are characterized by fascicles of spindle cells with moderate to abundant eosinophilic cytoplasm and elongated nuclei that can be hyperchromatic and pleomorphic. Frequent mitoses and foci of necrosis are also common. c-Kit/CD117, CD34, and DOG1 are always negative in leiomyosarcomas. These tumors label with desmin and smooth muscle actin.
Solitary fibrous tumor is a slow-growing spindle-cell neoplasm that can arise in a variety of soft tissue and visceral sites. Grossly, the tumor is solitary and well-circumscribed and can be multinodular. Hypocellular and hypercellular areas with staghorn vessels are common. Bundles of thick ropy collagen fibers are noted. Spindle cells often have minimal cytoplasm and elongated nuclei. Criteria for malignancy include infiltrative margins, necrosis, hypercellularity, nuclear atypia, pleomorphism, hyperchromasia, greater than 4 mitotic figures per 10 high-power fields, and atypical mitoses. Although CD34 is expressed in solitary fibrous tumors, these tumors do not label with c-Kit/CD117 or DOG1. CD99 and STAT6 labelling are also common.
Sclerosing mesenteritis is a paucicellular lobulated fibrotic lesion. It frequently affects the mesentery of the small and large bowel. The etiology is unknown, although some cases have been associated with IgG4-related sclerosis. Grossly, the lesion is not circumscribed; the involved mesentery feels thickened and firm. Histologic features include entrapped fat and fat necrosis, dense fibrosis with collagen deposition, and a chronic inflammatory infiltrate dispersed throughout the lesion. Similar to GIST, CD117 and CD34 can be expressed; however, an IgG4 immunostain would highlight cells in an IgG4-related case.
Supplementary Questions
- Which of the following is true regarding Gastrointestinal stromal tumor (GIST)?
- GIST most frequently arise in the esophagus
- Most GIST are associated with genetic syndromes
- Pediatric-age girls are affected more than boys
- Surgical resection is the only treatment option
- The vast majority demonstrate spindle-cell morphology
- Which of the following is a feature common to both GIST and abdominal fibromatosis?
- Both are spindle-cell neoplasms that affect women more frequently than men
- Both are spindle-cell neoplasms that demonstrate nuclear beta catenin labeling on immunohistochemistry
- Both are spindle-cell neoplasms that occur sporadically and are rarely associated with genetic syndromes
- Both are spindle-cell neoplasms with frequent necrosis and cystic changes
- Both are spindle-cell neoplasms with well-circumscribed borders
- A 66-year-old man has a duodenal GIST resected. Microscopic examination reveals that the 7 cm tumor demonstrates spindle-cell morphology. There are areas of necrosis and examination of 5mm2 of tumor reveals 10 mitotic figures. What is the risk of progression for this tumor?
- High
- Moderate
- Low
- None
- Very low
References
- Demetri GD, Benjamin RS, Blanke CD, et al. NCCN Task Force report: management of patients with gastrointestinal stromal tumor (GIST)--update of the NCCN clinical practice guidelines. NCCN Task Force. J Natl Compr Canc Netw. 2007;5 Suppl 2:S1-S29.
- Meshikhes AW, Al-Momen SA. Gastrointestinal autonomic nerve tumors: a clinical review. J Gastrointest Surg. 2015;19(6):1144-1156.
- Sanchez-Hidalgo JM, Duran-Martinez M, Molero-Payan R, et al. Gastrointestinal stromal tumors: a multidisciplinary challenge. World J Gastroenterol. 2018;24(18):1925-1941.
- Schaefer IM, Mariño-Enríquez A, Fletcher JA. What is new in gastrointestinal stromal tumor? Adv Anat Pathol. 2017;24(5):259-267.
Author
Safia N. Salaria, MD
Surgical Pathology Committee
Vanderbilt University Medical Center
Nashville, TN
Answer Key
- The vast majority demonstrate spindle-cell morphology (e)
- Both are spindle-cell neoplasms that occur sporadically and are rarely associated with genetic syndromes (c)
- High (a)

