- Home
- Member Resources
- Pathology Case Challenge
- Small Intestine
Clinical Summary
A 21-year-old woman presents with intractable severe abdominal pain with nausea and vomiting. The patient’s history is notable for a recent trip to Mexico, previous episodes of “upset stomach” and associated diarrhea over the past three to four years treated with a nonsteroidal anti-inflammatory drug (NSAID). Serologic and stool testing was unrevealing. Emergent partial resection of the jejunum is performed, with perforation identified intraoperatively. The gross exam demonstrates a segment of small intestine with a tan-hyperemic serosal surface, scattered tan-brown exudative material, with abundant near-circumferential adherent adipose tissue. There are two zones of luminal narrowing to a diameter of 1 cm. AFB and GMS staining is negative.
Master List of Diagnoses
- Crohn disease of the small intestine
- Intestinal tuberculosis
- NSAID-induced enteropathy
- Ulcerative colitis of the small intestine
- Yersiniosis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 39, and is Crohn disease of the small intestine.
The information provided in this case was accurate and correct at the time of publication in 2020. Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
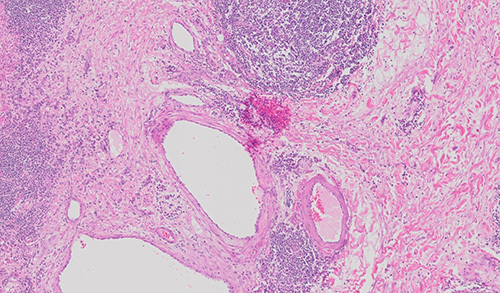
Microscopic evaluation of the resected small intestine demonstrates both superficial and deep lymphoid aggregates and loss of the normal villous architecture. There is a copious inflammatory infiltrate expanding the lamina propria composed of plasma cells, lymphocytes, and neutrophils. Areas of ulceration, cryptitis and crypt abscesses are present. Focal pyloric metaplasia is noted in the deep portion of the mucosa. There is full thickness lymphoid aggregates, increased fibrosis and scattered neural hyperplasia. The muscularis propria is mildly expanded, and inflammation extends to the serosal surface, with associated edema. The diagnosis is Crohn disease (CD) of the small intestine.
The incidence of CD is increasing worldwide. Men and women are equally affected, with most individuals presenting between the second and fourth decade of life, and a smaller subset presenting in the sixth decade. CD is a chronic, progressive, relapsing, and remitting inflammatory disorder that may involve any portion of the gastrointestinal (GI) tract, however, colon and terminal ileum are the most commonly affected with aphthous ulcers disrupting the mucosa with intervening segments of normal intestine (skip lesions). Mucosal damage may progress to strictures, fistulas, or abscesses in about 50% of the patients. Presentation and severity of the disease may vary. Common symptoms include abdominal pain, chronic diarrhea, melena, fatigue, anorexia, and weight loss. The etiology of CD has not been completely elucidated but appears to be immune-related involving genetic and environmental factors, with a likely role for intestinal bacteria. These factors work in a complex relationship to induce mucosal damage. CD is known to be more common in the Ashkenazi Jewish population and less frequent among individuals with African or Asian heritage. Several environmental factors such as a Western diet, smoking, antibiotic exposure in childhood, aspirin, NSAIDs, and oral contraceptives have all been linked to a higher incidence of CD.
CD may behave differently based on the affected portion of the GI tract. Of studied individuals, 15% - 35% of patients with CD have only small intestine involvement at the time of diagnosis. Unless the disease affects the terminal ileum, small intestine involvement is likely to be missed on colonoscopy. Approximately 10% of CD patients present with a perforating injury. CD of the jejunum is associated with an increased risk of relapse compared to with ileal CD. Strictures tend to occur more frequently in small intestinal than colonic CD. Interestingly, jejunal CD seems to be more common in the Asian population. Computerized tomography (CT), ultrasound, magnetic resonance enterography, and capsule endoscopy are promising modalities that may help better identify patients with small intestine CD.
On gross examination, CD classically demonstrates fat wrapping, serosal adhesions, fistulas, strictures, mucosa with a cobblestone appearance, erosions, and serpiginous ulcers. Microscopically, crypt architectural distortion, increased number of lamina propria lymphocytes and plasma cells, and transmural chronic inflammation is characteristic of the disease. There is also usually neutrophilic cryptitis and crypt abscesses. Pyloric metaplasia characterized by a replacement of the normal brush border and goblet cells with pyloric-type epithelium is typical of CD. Submucosal fibrosis, fissuring ulcers, transmural lymphoid aggregates, vasculitis, neuronal hypertrophy, and muscular hypertrophy may all be seen. Although epithelioid granulomas are considered the histologic hallmark of CD, they are only seen in approximately 15% of biopsies and 70% of resection specimens.
Intestinal tuberculosis (TB) is a mimicker of CD; it is an intestinal infection with Mycobacterium tuberculosis. This is an important entity to exclude before suggesting CD, particularly because CD and intestinal TB have radically different treatment protocols. To best identify this condition, clinical, radiographic, endoscopic, and histologic features should all be considered. Identification of travel to or residence in an endemic TB area should be the initial clue. Fever, night sweats, and pulmonary complaints are more common in intestinal TB, whereas diarrhea, weight loss, hematochezia, perianal disease, a history of an appendectomy, and longer symptom duration favor a diagnosis of CD. On CT, intestinal TB tends to show asymmetric thickening of the intestine wall and preferential involvement of the terminal ileum, ileocecal valve and right colon. Radiographic involvement of the left side of the colon and rectum and symmetric wall thickening is more compatible with CD. Endoscopically, intestinal TB is more likely to show transverse ulcers, as opposed to the longitudinal and aphthous ulcers and cobblestone mucosal appearance of CD. l. On microscopy, intestinal TB more often contains necrotizing, confluent granulomas. Unfortunately, acid-fast stains have low sensitivity and specificity in identifying TB. Additional studies, such as interferon gamma release assays, may be employed by the clinical team in situations where the diagnosis of TB remains uncertain.
NSAID-induced enteropathy is a condition where NSAID use produces ulceration leading to significant bleeding, obstruction, or perforation in the small intestine. A rare subset of this ailment is known as diaphragm disease, characterized by luminal narrowing due to extensions of multiple mucosal septa in a web-like distribution. As many as 71% of long-term NSAID users experience small intestinal damage. Up to 8.4% of NSAID users in one study were found to possess small intestinal ulceration. Nevertheless, this damage may be subclinical or present with vague symptomatology. The pathogenesis remains unclear but appears to be multifactorial. NSAID-induced enteropathy may appear similar to CD endoscopically, with scattered aphthous ulcers. The histologic features of the enteropathy are broad and comprise mild erosions to deep ulcers with accompanying neutrophilic infiltrates. However, pyloric metaplasia, architectural distortion and intense plasma cell infiltrates are unusual in NSAID-induced enteropathy and are more consistent with a diagnosis of CD.
Ulcerative colitis (UC) of the small intestine, outside of “backwash ileitis,” is incredibly unusual and should prompt a search for features of CD, drug-induced injury and infection. UC typically shows chronicity and activity affecting the superficial portion of the intestine (mucosa and superficial submucosa). These changes classically involve the distal large intestine in a continuous fashion, decreasing in severity proximally. In cases of ulcerative pancolitis, patients may demonstrate a mild amount of active inflammation characterized by patchy cryptitis or crypt abscesses with villous atrophy in the distal one or two centimeters of the terminal ileum. This is known as “backwash ileitis” because it is thought to occur by colonic contents seeping back through an incompetent ileocecal valve. The phenomenon has been observed in instances that lack cecal involvement or discontinuous ileal involvement. This has prompted some to suggest backwash ileitis may be a manifestation of intestine preparation or drug effect.
Yersiniosis is a known mimicker of CD and can cause gastrointestinal bleeding and even perforation. Although typically a self-limited process, the immunocompromised, debilitated patients, and those with elevated iron levels are at highest risk for severe yersiniosis. In the intestines, yersiniosis is most often caused by Yersinia enterocolitica or Yersinia pseudotuberculosis and most commonly affects the ileum, appendix, and right colon. If severe, this process may appear similar to CD radiographically. Microscopically, this disease produces ulcers, cryptitis, necrotizing granulomas or epithelioid granulomas with a lymphoid cuff and transmural lymphoid aggregates. However, features of chronicity such as neural hyperplasia, crypt architectural distortion and thickening of the muscularis mucosae are unusual and are more in keeping with CD. Serologic and stool test may be used in suspected cases to confirm the presence of Yersinia; such testing was negative in this case.
Supplementary Questions
- Which of the following histologic descriptions is most characteristic of Crohn disease?
- An isolated deep mucosal ulceration and associated cryptitis without crypt distortion or pyloric metaplasia
- Edematous mucosa with widespread superficial erosions and ulcerations
- Necrotizing granulomatous inflammation
- Mucosal erosions with adjacent malformed crypts in a background of increased plasma cells and transmural lymphoid aggregates
- Mucosal ulcers, cryptitis, and large necrotizing granulomas
- What is the leading cause of Diaphragm disease?
- Crohn disease of the small intestine
- Intestinal tuberculosis
- Nonsteroidal anti-inflammatory drug-induced enteropathy
- Ulcerative colitis of the small intestine
- Yersiniosis
- Which finding most strongly suggests a diagnosis of Crohn disease over yersiniosis?
- Crypt architectural distortion
- Cryptitis
- Granulomas
- Transmural lymphoid aggregates
- Ulceration
References
- Azghari I, Bargach A, Billah NM, Essaoudi MA, Jahid A, Kabbaj N. Ileocecal resection for massive rectal bleeding due to Yersinia enterocolitica: a case report and review of the literature. J Med Case Rep. 2016;10:1-6.
- Fong SC, Irving PM. Distinct management issues with Crohn’s disease of the small intestine. Curr Opin Gastroenterol. 2015;31(2):92-97.
- Odze RD, Goldblum JR. Surgical Pathology of the GI tract, liver, biliary tract, and pancreas. 3rd ed. Philadelphia, PA: Elsevier Saunders. 2015;67, 232, 418-419, 422-428, 447, 471.
- Peyrin-Biroulet L, Loftus EV, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105(2):289-297.
- Shin SJ, Noh CK, Lim SG, Lee KM, Lee KJ. Non-steroidal anti-inflammatory drug-induced enteropathy. Intest Res. 2017;15(4):446-455.
- Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet, L. Crohn’s disease. Lancet. 2017;389(10080):1741-1755.
- Woodman I, Schofield JB, Haboubi N. The histopathological mimics of inflammatory intestine disease: a critical appraisal. Tech Coloproctol. 2015;19(12):717-727.
Answer Key
- Mucosal erosions with adjacent malformed crypts in a background of increased plasma cells and transmural lymphoid aggregates (d)
- Nonsteroidal anti-inflammatory drug-induced enteropathy (c)
- Crypt architectural distortion (a)

