Clinical Summary
A 60-year-old woman presents with fatigue and a 20-pound weight loss. Her past medical history is unremarkable. Endoscopy reveals an 8 cm ulcerated mass located in the gastric antrum. She subsequently undergoes a distal subtotal gastrectomy.
Master List of Diagnoses
- Gastric carcinoma with lymphoid stroma
- Gastrointestinal stromal tumor
- Metastatic lobular carcinoma (breast)
- Poorly differentiated gastric adenocarcinoma
- Signet ring lymphoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 18, and is poorly differentiated gastric adenocarcinoma (stomach).
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case
Criteria for Diagnosis and Comments
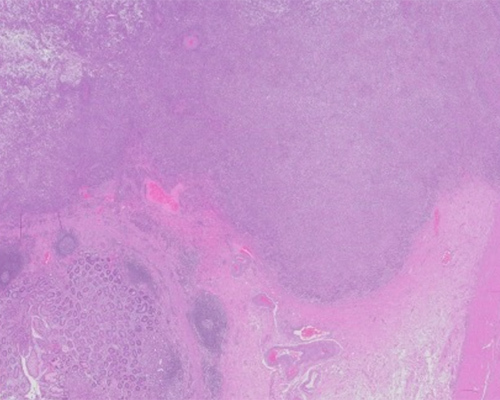
The representative sections demonstrate small groups and isolated malignant cells with areas of sheet-like growth infiltrating into the muscularis propria. Some foci of distinct gland formation are present. A subset of cells exhibits conspicuous intracytoplasmic mucin and eccentrically located nuclei, while the majority of cells have more centrally placed nuclei and amphophilic cytoplasm. The nuclei demonstrate moderate pleomorphism with coarse chromatin and scattered prominent nucleoli. Tumor cells floating within mucin are present but represent less than 50% of the tumor volume. The background gastric mucosa is notable for chronic lymphoplasmacytic inflammation with intestinal metaplasia. These findings are consistent with a diagnosis of poorly differentiated gastric adenocarcinoma and could be classified as a mixed-type carcinoma by the Laurén and World Health Organization (WHO) classification schemes.
Gastric cancer is a heterogeneous group of tumors with multifactorial etiologies along with varied morphologies, anatomic distribution, and mutational profiles. Gastric cancer is the second most common cancer worldwide, and despite falling mortality and incidence rates, it is a leading cause of cancer-related deaths. In parts of Asia, gastric cancer is endemic, accounting for more than half of the approximately 1 million cases that develop per year globally
Gastric cancer is rare before the age of 40 and peaks in the 7th decade of life. Risk factors include Helicobacter pylori infection, dietary factors (eg, high salt intake and low consumption of fruits and vegetables), cigarette smoking, obesity, and bile reflux. H. pylori is the most common chronic bacterial infectious agent in humans, with greater than 50% of the world population infected. Numerous studies have shown H. pylori infection to significantly increase the risk of gastric carcinomas; it is now recognized as an established cause of gastric cancer.
Gastric carcinomas have been classified by both gross and microscopic features. The most commonly used microscopic schemes are the Laurén and WHO systems. The Laurén classification system, published in 1965, divides carcinomas into intestinal, diffuse, mixed, and indeterminate types. The WHO system subtypes gastric adenocarcinoma into tubular adenocarcinoma, parietal cell carcinoma, adenocarcinoma with mixed subtypes, papillary adenocarcinoma NOS, micropapillary carcinoma NOS, mucoepidermoid carcinoma, mucinous adenocarcinoma, signet-ring cell carcinoma, medullary carcinoma with lymphoid stroma, hepatoid adenocarcinoma, paneth cell carcinoma, and poorly cohesive carcinoma.
Tubular and papillary types are generally considered to be subvariants of the Laurén intestinal type, characterized by cohesive growth and gland formation. Poorly cohesive and diffuse type-carcinomas, of which signet-ring cell carcinoma is the archetype, lack gland formation and are composed of cells that are isolated or arranged in small aggregates. Grading applies primarily to tubular and papillary carcinomas; though diffuse-type carcinomas are often graded as poorly differentiated or high-grade. Literature comparing these classifications as independent prognostic features is conflicting, and the most meaningful prognostic indicators relate to extent of tumor and presence of regional lymph node metastases.
Intestinal-type gastric carcinoma, most often located in the antro-pyloric region, typically arises in a background of chronic gastritis and intestinal metaplasia and in most cases is associated with H. pylori infection. The multistep process that progresses from H. pylori infection to atrophy, intestinal metaplasia, dysplasia, and eventually intestinal-type carcinoma is known as the Correa cascade of gastric carcinogenesis. In addition, intestinal-type carcinoma is the most common histological variant found in the proximal stomach. Carcinomas of the proximal stomach have had a dramatic increase in incidence over the last few decades in the US, similar to distal esophageal adenocarcinomas, and appear to share similar risk factors, such as gastroesophageal reflux disease and obesity.
Diffuse-type carcinoma often arises in the body, is less often preceded by intestinal metaplasia, and is associated with H. pylori infection to a lesser extent in some studies. Often cases of diffuse-type carcinoma will have no discrete mass and can manifest as plaque-like lesions or as diffuse gastric thickening and stiffness secondary to extensive wall infiltration known as linitis plastica.
While the majority of gastric carcinomas are sporadic, about 10% have an inherited familial component. Germline mutations in the CDH1 gene encoding E-cadherin, a cell adhesion protein, lead to hereditary diffuse gastric carcinoma (HDGC). HDGC is inherited in an autosomal dominant fashion, with a penetrance of approximately 70% and an age of onset as young as 14 years. Gastric carcinoma arising in patients with HDGC are diffuse-type, often with signet-ring cells. Other syndromes with an increased risk of developing gastric carcinomas include Lynch syndrome, familial adenomatous polyposis, Li–Fraumeni syndrome, and Peutz–Jeghers syndrome.
The prognosis for patients with gastric carcinoma is most strongly related to stage at diagnosis. Early gastric cancer (EGC), defined as invasive carcinoma confined to the mucosa or submucosa, has a good prognosis after resection, with reported 5-year survival rates greater than 90%. In the Western world, EGC accounts for only 15% - 21% of newly diagnosed gastric cancers. In areas with mass screening programs, such as Japan, EGC represents greater than 50% of gastric cancers. Advanced gastric carcinomas (ie, tumors invading the muscularis propria or beyond) follow a more aggressive course, not uncommonly presenting with hematemesis and symptoms of gastric outlet obstruction at presentation. Prognosis of advanced gastric carcinoma ranges from 65% - 81% 5-year survival for tumors confined to the muscularis propria, and 16% for patients with pT4 disease.
Treatment depends on accurate staging of the extent of disease. Preoperative staging may include chromoendoscopy, endoscopic ultrasound, computed tomography scans of the abdomen and chest, positron emission tomography, and staging laparoscopy. EGC may be amendable to advanced endoscopic techniques such as endoscopic mucosal resection and endoscopic submucosal dissection. Advanced gastric carcinomas, and a subset of EGCs, are treated by resection with or without adjuvant or perioperative chemotherapy or chemoradiotherapy.
Human epithelial growth factor receptor 2 (HER2) gene amplification was described in gastric carcinoma after its discovery in breast cancer. HER2 overexpression is found in approximately 20% of gastric carcinomas, more often in intestinal-type carcinoma and in carcinomas of the proximal stomach. The large-scale international ToGA trial showed that a humanized monoclonal antibody against HER2, trastuzumab, when combined with chemotherapy (fluoropyrimidine/cisplatin), could prolong overall and progression-free survival in HER2-positive advanced gastric carcinoma (ie, HER2 3+ by immunohistochemistry or HER2 fluorescence in situ hybridization [FISH] amplified). FDA approval for trastuzumab was granted for patients with HER2-positive metastatic adenocarcinoma of stomach or gastroesophageal junction. Based on these findings, it is recommended that all patients with advanced gastric or gastroesophageal carcinoma be tested for HER2 by immunohistochemistry and/or FISH at initial diagnosis.
Gastric carcinomas with lymphoid stroma (medullary carcinoma or lymphoepithelioma-like carcinoma) have a predilection for the proximal stomach and are composed of poorly differentiated cells with sheet-like or tubular growth embedded in a prominent lymphocytic infiltrate. Greater than 80% of these tumors are associated with Epstein–Barr virus infection, which can be detected by EBV-encoded small RNA in-situ hybridization (EBER ISH). Some may also be associated with microsatellite instability. The outcome is reportedly better than for typical adenocarcinoma.
Gastrointestinal stromal tumors (GISTs) with epithelioid features may rarely enter the differential with gastric carcinoma, particularly when they involve the lamina propria. Features supportive of carcinoma include gland formation and marked pleomorphism. Of note, focal cytokeratin immunoreactivity has been reported in a small fraction of epithelioid GISTs. Immunohistochemical positivity for CD117 or DOG1 would confirm a diagnosis of GIST.
Metastatic tumors to the stomach, though uncommon, can clinically mimic a primary carcinoma. Melanoma and malignancies originating from the breast, lung and kidney are the most commonly reported tumors to metastasize to the stomach. Metastatic lobular carcinoma can be particularly problematic, due to its characteristic single-file growth pattern and ability to involve the stomach diffusely, mimicking linitis plastica. A panel of immunohistochemical stains including ER, GATA3, cytokeratin 20, and CDX2 have proven useful in discriminating gastric from breast origin.
Signet ring cell morphology has been reported in both B- and T-cell non-Hodgkin lymphomas, as well as plasma cell neoplasms, mostly as single case reports. Focal cohesive growth and the identification of even rare glands favor carcinoma. A basic panel of immunohistochemical stains (eg, pankeratin and CD45) can help establish a diagnosis.
Supplementary Questions
- Which of the following is true regarding gastric carcinoma?
- HER2 testing is not recommended for advanced gastric carcinoma.
- Histologic subtype is more important than staging for prediction of survival.
- In North America and European countries, it is most often caught at an early stage.
- It is a genetically and histologically homogenous group of tumors.
- Its incidence is decreasing worldwide.
- Which of the following risk factors for distal gastric carcinoma is likely responsible for the most cases worldwide?
- Autoimmune gastritis
- Bile reflux
- Diet
- Helicobacter pylori infection
- Smoking
- WWhat gene is most commonly mutated in hereditary cases of gastric carcinoma?
- APC
- CDH1
- CTNNA1
- MUTYH
- STK11
References
- Hayakawa Y, Sethi N, Sepulveda AR, Bass AJ, Wang TC. Oesophageal adenocarcinoma and gastric cancer: Should we mind the gap? Nat Rev Cancer. 2016;16(5):305-318.
- Hui Y, Wang Y, Nam G, et al. Differentiating breast carcinoma with signet ring features from gastrointestinal signet ring carcinoma: assessment of immunohistochemical markers. Hum Pathol. 2018;77:11–19.
- Ku GY, Ilson DH. Cancer of the stomach. In: Niederhuber JE, Armitage JO, Kastan MB, Doroshow JH, Tepper JE, eds. Abeloff's clinical oncology. 6th ed. Elsevier; 2020: 1197-1210.
- Lokuhetty D, White VA, Watanabe R, Cree IA. eds. WHO Classification of Tumours of the Digestive System. 5th ed. IARC Press; 2019.
- Lauwers GY. Epithelial neoplasms of the stomach. In: Odze RD, Goldblum JR, Crawford JM, eds. Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas.2nd Ed. Saunders; 2009:563-579.
- O’Connell FP, Wang HH, Odze RD. Utility of immunohistochemistry in distinguishing primary adenocarcinomas from metastatic breast carcinomas in the gastrointestinal tract. Arch Pathol Lab Med. 2005;129(3):338–347.
- Surveillance, Epidemiology, and End Results (SEER) Program. Cancer Stat Facts: Stomach Cancer. https://seer.cancer.gov/statfa.... Accessed April 1, 2019.
- Zhang S, Sun J, Fang Y, et al. Signet-ring cell lymphoma: clinicopathologic, immunohistochemical, and fluorescence in situ hybridization studies of 7 cases. Ann Diagn Pathol. 2017;26:38-42.
Answer Key
- Its incidence is decreasing worldwide. (e)
- Helicobacter pylori infection (d)
- CDH1 (b)

