- Home
- Member Resources
- Pathology Case Challenge
- Left Flank
Clinical Summary
A 47-year-old woman presents with a 12 cm left flank mass. Computed tomography scan shows a deep seated homogenous well-circumscribed mass. The resected mass shows a yellow-tan lobular soft cut surface.
Master List of Diagnoses
- Atypical lipomatous tumor/well-differentiated liposarcoma (ALT/WDL)
- Fat necrosis
- Hibernoma
- Lipoma
- Normal fat
- Spindle cell lipoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 39, and is a lipoma in the left flank.
Criteria for Diagnosis and Comments
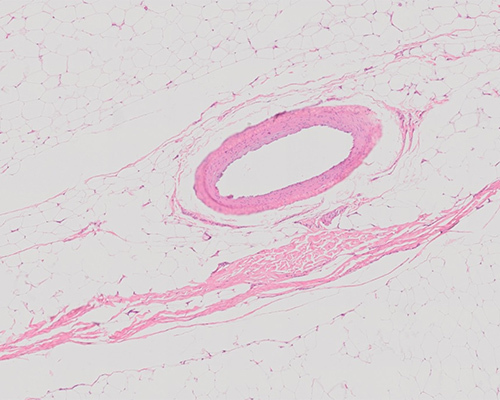
H&E-stained sections show sheets of mature adipocytes with no cytologic atypia, hyperchromasia, or pleomorphism, consistent with lipoma. No spindle cell features or wavy collagen fibers are present.
At least 30% of benign tumors of soft tissue are lipomas. Conventional lipomas can be in superficial or deep soft tissue (usually within subcutaneous tissue and generally smaller than 5 cm), but so-called giant lipomas similar to this case can occur anywhere in the body. Clinically, lipomas present as a painless soft tissue mass; however, larger tumors can be painful due to compression of peripheral nerves. Lipomas can be multiple. On imaging studies, they are homogenous soft tissue masses, iso-dense to fat.
Grossly, lipomas are relatively well-circumscribed, with a thin capsule and a yellow, greasy and lobular cut surface. Histologically, they are characterized by mature adipocytes with no cytologic atypia, hyperchromasia, or pleomorphism. In small samples, adipocytes of a lipoma are often indistinguishable from those of normal, non-lesional fat.
Lipomas can occasionally have bone formation (osteolipoma), cartilage (chondrolipoma), abundant fibrous tissue (fibrolipoma), or abundant myxoid areas (myxolipoma). The subclassification of lipomas does not seem to have any prognostic value. Lipomas stain for S100 protein, leptin, and HMGA1. They are negative for protein expression of MDM2 and CDK4, and MDM2 is not amplified. On ultrastructural examination, the neoplastic cells have a single lipid droplet compressing a peripherally situated nucleus. The majority of lipomas have an abnormal karyotype, the most common aberrations involving 12q13-15. Cytogenetic studies are warranted for: large (>10 to 15 cm in diameter) fatty tumors deep within the extremities of patients >50 years of age, recurrent fatty tumors, retroperitoneal/pelvic/abdominal fatty tumors, or lipomatous tumors with “equivocal” cytologic atypia as these tumors most likely represent atypical lipomatous tumor/well-differentiated liposarcoma
Spindle cell lipoma (SCL) and pleomorphic lipoma (PL) are subtypes of lipoma that can mimic ALT/WDL. Clinically, these are well-defined, asymptomatic, subcutaneous masses that grow slowly over the years. The size usually ranges from 3 to 5 cm, and they predominantly occur in the shoulder/neck region of older men. The histologic features vary significantly between cases, but the lesions are generally located superficial to fascia.
The classic SCL is composed of a mixture of spindle cells and mature adipocytes, myxoid stroma, and wiry collagen. Spindle cells display an elongated nucleus, an enlarged and bipolar cytoplasm, a small nucleolus and scarce mitotic figures. The cells may focally tend to group in parallel bands with the nuclei arranged in palisades, similar to schwannoma. Foci of osseous or cartilaginous metaplasia may be seen.
The classic PL is characterized by the presence of bizarre multinucleated cells (floret cells) with several hyperchromatic and multinucleated nuclei and eosinophilic cytoplasm scattered throughout the lesions. There are also short, birefringent collagen bundles; clusters of lymphocytes and plasma cells; and myxoid stroma. Phenotypically, SCL and PL cells express CD34 and often bcl2 but are negative for actin and desmin. S100 is negative in spindle cells and floret cells. SCL/PL is characterized by partial or whole chromosome 13 and/or 16 deletions.
The nomenclature of atypical lipomatous tumor/well-differentiated liposarcoma (ALT/WDL) has been changing over the last few decades. Prior to 1979, all cases were diagnosed as WDL regardless of depth and location. Per the current World Health Organization classification, “atypical lipomatous tumors” in any locations are to be considered mesenchymal tumors of intermediate (borderline) malignancy. However, the most commonly used nomenclature is “ALT” for superficial and intramuscular tumors in extremities and “WDL” for inguinal, para-testicular, retroperitoneal, and mediastinal tumors. ALT/WDL is the most common liposarcoma in adults, with a peak incidence during the fifth and sixth decades and no sex predilection. ALT/WDL usually lacks metastatic potential but can recur frequently. The degree of recurrence and its aggressiveness depend largely on topographic tumor location.
In general, ALT/WDL is larger and not as sharply circumscribed as a lipoma. ATL/WDL is histologically characterized by the presence of a mixed population of lipoblasts and lipocytes but more importantly by cells with atypical hyperchromatic pleomorphic nuclei. These tend to be more commonly found near blood vessels and within fibrous septa. Phenotypically, most mature lipoblasts and adipocytes of ALT/WDL express S100 protein. ALT/WDL can be distinguished from benign adipocytic neoplasms by its positivity for p16, CDK4 and MDM2. Cytogenetically, supernumerary giant chromosomes and ring chromosomes (revealing amplified sequences of 12q14-15, which correlate with the MDM2, HMGA2, YEATS4, CDK4, and CPM genes, among others) are the most characteristic abnormalities.
Fat necrosis is often secondary to trauma and is characterized by foamy macrophages and occasionally multinucleated giant cells with foamy cytoplasm, fragments of normal as well as degenerating adipose tissue, and sparse and variable numbers of other inflammatory cells in a granular background. It may show irregular fibrous septae, adipocyte size variability, and enlarged lipid-laden histiocytes, mimicking lipoblasts. The normal capillary vasculature of fat may become more prominent due to shrinkage of fat cells. MDM2 protein expression by immunohistochemistry may also be seen aberrantly in fat necrosis.
Hibernoma often occurs in younger patients than conventional lipoma. They occur most commonly in the thigh but can occur in a variety of sites. Clinically, it presents as a solitary, 5 to 15 cm, asymptomatic, slow-growing, subcutaneous mass, which was probably present for many years before excision. Four histologic variants, including classic, myxoid, lipoma-like, and spindle cell variants have been described. Histologically, the most common variant is classic hibernoma, which shows a lobular proliferation of cells with variable degrees of differentiation (monotonous, round, or ovoid) with eosinophilic granular cytoplasm containing multiple Oil Red O-positive lipid vacuoles and a small central nucleus (multi-vacuolated brown fat cells, mimicking lipoblasts). Lipoma-like hibernoma can have predominant white fat with focal areas of brown fat. Karyotypic aberrations involving 11q13-21 have been described as the most common chromosomal abnormality.
Normal fat shows sheets of mature adipocytes with varying size and no cytologic atypia.
Supplementary Questions
- Which of the following is the most characteristic immunohistochemical profile of lipomas?
- MDM2-, CDK4-
- MDM2-, CDK4+
- MDM2+, CDK4-
- MDM2+, CDK4+
- MDM2+, p16+
- Which of the following may shows MDM2 protein IHC expression?
- Fat necrosis
- Hibernoma
- Normal fat
- Pleomorphic lipoma
- Spindle cell lipoma
- Which of the following is the most related with the degree of recurrence and aggressiveness of atypical lipomatous tumor/well-differentiated liposarcoma?
- Age of the patient
- Gender of the patient
- Location of tumor
- Presence of osseous or cartilaginous metaplasia
- Size of tumor
References
- Enzinger FM, Harvey DA. Spindle cell lipoma. Cancer. 1975;36(5):1852-1859.
- Fletcher CD, Akerman M, Dal Cin P, et al. Correlation between clinicopathological features and karyotype in lipomatous tumors. A report of 178 cases from the Chromosomes and Morphology (CHAMP) Collaborative Study Group. Am J Pathol. 1996;148(2):623-630.
- Meis-Kindblom JM, Sjögren H, Kindblom LG, et al. Cytogenetic and molecular genetic analyses of liposarcoma and its soft tissue simulators: recognition of new variants and differential diagnosis. Virchows Arch. 2001;439(2):141-151.
- Mentzel T, Fletcher CD. Dedifferentiated myxoid liposarcoma: a clinicopathological study suggesting a closer relationship between myxoid and well-differentiated liposarcoma. Histopathology. 199730(5):457-463.
- Requena L, Kutzner H. Cutaneous Soft Tissue Tumors. 1st edition. Alphen aan den Rijn, Netherlands: Wolters Kluwer. 2015; 844-849, 859-867.
- Rosai J, Akerman M, Dal Cin P, et al. Combined morphologic and karyotypic study of 59 atypical lipomatous tumors. Evaluation of their relationship and differential diagnosis with other adipose tissue tumors (a report of the CHAMP Study Group). Am J Surg Pathol. 1996;20(10):1182-1189.
- Rosso R, Lucioni M. Normal and neoplastic cells of brown adipose tissue express the adhesion molecule CD31. Arch Pathol Lab Med. 2006;130(4):480-482.
- Rubin BP, Dal Cin P. The genetics of lipomatous tumors. Semin Diagn Pathol. 2001;18(4):286-293.
- Shmookler BM, Enzinger FM. Pleomorphic lipoma: a benign tumor simulating liposarcoma. A clinicopathologic analysis of 48 cases. Cancer. 1981;47(1):126-133.
Authors
Viren Patel, MD
Surgical Pathology Fellow
UT MD Anderson Cancer Center
Houston, TX
Phyu P Aung, MD, PhD, FCAP
Surgical Pathology Committee
UT MD Anderson Cancer Center
Houston, TX
Answer Key
- MDM2-, CDK4- (a)
- Fat necrosis (a)
- Location of tumor (c)