Clinical Summary
An 82-year-old woman presents with vague abdominal pain and increasing jaundice. Her medical history is notable for primary sclerosing cholangitis. Radiology reveals a right liver lobe mass. Gross examination of the hepatectomy specimen shows green to yellow mottled parenchyma with a 7.5 cm firm tan nodule. Of note, the gallbladder and extrahepatic bile ducts are unremarkable on gross and histologic examination.
Master List of Diagnoses
- Bile duct adenoma
- Focal nodular hyperplasia
- Hepatocellular carcinoma
- Intrahepatic cholangiocarcinoma
- Metastatic colonic adenocarcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 06, and is intrahepatic cholangiocarcinoma of the liver.
Criteria for Diagnosis and Comments
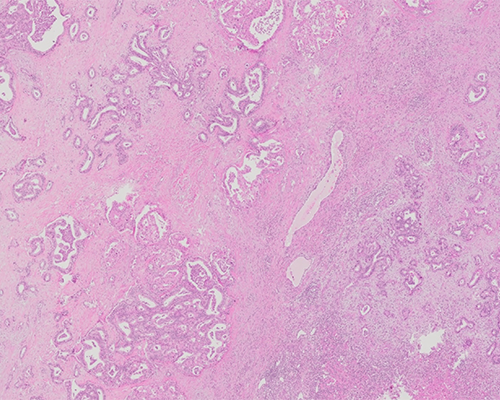
The histological sections demonstrate a circumscribed hepatic parenchymal lesion that is comprised of variably shaped glands embedded in a fibrotic stroma. The cells are cuboidal to columnar showing moderate pleomorphism. The cytoplasm ranges from densely eosinophilic to pale. The nuclei are large with clumped chromatin. The neoplastic glands are invading a very fibrotic stroma with patchy inflammation. Some foci of single cells infiltrating through the stroma are noted. The background liver shows portal inflammation that is consistent with mass effect; however, it is not cirrhotic. These findings are consistent with a diagnosis of intrahepatic cholangiocarcinoma.
Intrahepatic cholangiocarcinoma (ICC) is defined as an intrahepatic malignancy with biliary epithelial differentiation. It comprises 10% of primary liver malignancies. The World Health Organization (WHO) is favoring that the term cholangiocarcinoma incorporates intrahepatic tumors with biliary differentiation. Any portion of the intrahepatic biliary network can give rise to this tumor. The age specific incidence is highest in patients over 85 years. It is more commonly encountered in men and has an increased incidence in Southeast Asian countries. Biliary and hepatic diseases such as primary sclerosing cholangitis, hepatolithiasis, parasitic infection of the biliary tract (liver flukes Clonorchis sinensis or Opisthorchis viverri), biliary malformations, and non-biliary causes of cirrhosis (eg, viral hepatitis) are all risk factors for ICC. Hereditary hemochromatosis and exposure to Thorotrast and the Epstein-Barr virus have also been implicated in the etiology of ICC.
Solitary ICCs can range in size from 7.0 to 10.0 cm; multinodular disease is often diffuse and comprised of multiple sub-centimeter lesions. ICCs are classified into three subtypes: (1) the mass-forming type presenting as a solitary parenchymal lesion that is greyish-white in color and firm in consistency, (2) periductal infiltrating ICC affecting portal tracts, causes narrowing of involved bile ducts, cholangitis, and an obstructive pattern of injury, and (3) the intraductal growth pattern subtype of ICC representing malignant transformation of the intraductal papillary neoplasm of the bile duct, characterized by a dilated duct with luminal polypoid projections of tumor. Mass forming type accounts for 65% of all ICCs, while PI and IG type, represent 6% and 4% of all ICCs, respectively.
ICCs often arise in association with biliary intraepithelial neoplasia. A majority of ICCs are adenocarcinomas. The neoplastic cells are columnar/cuboidal and form variably sized tubular structures that resemble bile ducts-forming acinar, cord-like or papillary patterns of growth. The nuclei are round and centrally located. The glands are surrounded by acellular fibrous stroma with variable amounts of inflammation. Adenosquamous, squamous, clear cell, signet ring cell, lymphoepithelioma-like, mucinous, and sarcomatous histologic variants have been described. Mucin stains (mucicarmine, diastase-periodic acid Schiff, alcian blue) stains are positive in the tumor. Cytokeratin 7 and 19 are often expressed by the neoplastic cells as are carcinoembryonic antigen and epithelial membrane antigen.
ICC is an aggressive cancer that carries a poor prognosis. ICCs typically spread by direct invasion, along hepatic plates and nerves. Lymph node involvement (which is common at the time of presentation), vascular invasion, tumor at surgical resection margins, bilobar involvement, poor histologic differentiation, and MUC5AC expression in the tumor are associated with an unfavorable outcome. Surgery combined with adjuvant or neoadjuvant therapies are the standard of care, however, this is not curative for most patients. The American Cancer Society reports a 5-year survival for localized intrahepatic cholangiocarcinoma of 15% and a 2% 5-year survival for metastatic disease.
Hepatocellular carcinoma (HCC) is a malignant hepatocellular tumor. Differentiation is allotted based on how well the neoplastic cells recapitulate hepatocytes. There is variation in both the architectural growth patterns and the degree of cytologic atypia. Neoplastic cells have abundant to moderate amounts of cytoplasm; the cytoplasm can be pink with Mallory hyaline or show fatty or clear cell change. Large round nuclei and prominent nucleoli are common. Solid, trabecular, and pseudoglandular growth patterns are frequently encountered. The presence of arteries unaccompanied by portal tracts is a common feature of HCCs.
HCC is usually easily recognized on routine H&E stains; however, histochemical and immunostains can act as an adjunct to diagnosis. The diffuse expansion and/or loss of reticulin staining are frequent in hepatocellular carcinoma. CAM5.2 is positive in all HCCs. CD10 and polyclonal carcinoembryonic antigen are expressed by up to 90% of HCCs. CD34 shows a strong diffuse sinusoidal staining pattern in HCCs. HepPar1 has shown increased sensitivity for well to moderately differentiated HCCs. Glypican 3 labels up to 85% of HCCs and does not stain a non-inflamed and non-cirrhotic background liver. Overall, it is best to use a panel of markers when the diagnosis in in doubt.
Bile duct adenomas are benign subcapsular proliferations of small-sized bile ducts. They are usually solitary and less than 1.0 cm in size. The lesions are well-circumscribed and non-encapsulated and are comprised of glands with compressed lumens and lined by small uniform cuboidal cells with small nuclei. The bile duct proliferations are embedded in dense fibrous stroma. Mitoses and nuclear pleomorphism are not present.
Focal nodular hyperplasia is a benign condition that develops as result of shunting of arterial blood flow, which leads to the production of fibrous bands. Histologically, the lesion is comprised of nodules of benign hepatocytes with intervening thin fibrous septae. Reticulin staining demonstrates normal thickness (1 to 2 cells) hepatocyte trabeculae. Ductular reaction can be seen in the fibrous septae. The background liver is non-cirrhotic. Glutamine synthetase demonstrates map-like staining which can help differentiate focal nodular hyperplasia from inflammatory hepatic adenoma, which often shows diffuse staining.
Metastatic adenocarcinoma involving the liver cannot always be distinguished from ICC. The most common primary malignancies that metastasize to the liver are breast, colorectal, and gastric cancers. The presence of dysplasia in the intrahepatic bile ducts favors ICC. Metastases from colorectal adenocarcinomas are comprised of glands lined by tall columnar cells with prominent luminal necrosis. ICC typically will not express CK20 and CDX2. Metastatic breast adenocarcinoma will often express gross cystic disease fluid protein (GCDFP), estrogen receptor (ER), and progesterone receptor (PR). The cells are often arranged in nests of neoplastic cells with intracytoplasmic mucin. Lung carcinomas that metastasize to the liver will label with TTF-1, neuroendocrine tumors of the lung additionally label with synaptophysin and chromogranin. The immunohistochemical profiles of pancreatic and extrahepatic biliary adenocarcinomas show overlap with ICCs and clinic-radiographic findings may help in distinguishing the two.
Supplementary Questions
- Which of the following is true regarding intrahepatic cholangiocarcinoma (ICC)?
- Clonorchis sinensis and Opisthorchis viverri infection are important risk factors.
- Metastatic adenocarcinomas from non-hepatic primary tumors are easily distinguished from ICCs.
- Surgery is curative and the prognosis is excellent.
- The lesion develops as a result of shunting of arterial blood flow, which leads to the production of fibrous bands around nodules of hepatocytes.
- The tumor is most often comprised of multifocal subcentimeter lesions.
- Which of the following immunohistochemical and histologic features support a diagnosis of metastatic colorectal adenocarcinoma to the liver over ICC?
- CK20 and CDX2 positive variable sized columnar cell lined glands with abundant luminal necrosis
- CK7 and CK19 positive glands of cuboidal cells with clear to eosinophilic cytoplasm embedded in fibrotic stroma
- ER, PR, and GCDFP positive tumor cells arranged in nests with intracytoplasmic mucin
- Hep Par-1 and glypican 3 positive plates of polygonal cells with eosinophilic granular cytoplasm
- TTF-1, synaptophysin, and chromogranin positive tumor cells with salt and pepper chromatin
- Which of the following is a histologic feature of focal nodular hyperplasia?
- Expanded hepatic plates of cells with marked pleomorphism
- Glands lined by tall columnar cells with prominent luminal necrosis
- Nodules of benign hepatocytes with thin intervening fibrous septae
- Scattered lymphoid aggregates within the hepatic parenchyma
- Variably sized pleomorphic bile ducts
References
- Blechacz B. Cholangiocarcinoma: current knowledge and new developments. Gut Liver. 2017;11(1):13-26.
- Doherty B, Nambudiri VE, Palmer WC. Update on the Diagnosis and Treatment of Cholangiocarcinoma. Curr Gastroenterol Rep. 2017;19(1):2.
- Ebata T, Ercolani G, Alvaro D, Ribero D, Di Tommaso L, Valle JW. Current Status on Cholangiocarcinoma and Gallbladder Cancer. Liver Cancer. 2016;6(1):59-65.
- Vijgen S, Terris B, Rubbia-Brandt L. Pathology of intrahepatic cholangiocarcinoma. Hepatobiliary Surg Nutr. 2017;6(1):22-34.
Author
Safia N. Salaria, MD
Surgical Pathology Committee
Vanderbilt University Medical Center
Nashville, TN
Answer Key
- Clonorchis sinensis and Opisthorchis viverri infection are important risk factors. (a)
- CK20 and CDX2 positive variable sized columnar cell lined glands with abundant luminal necrosis (a)
- Nodules of benign hepatocytes with thin intervening fibrous septae (c)