- Home
- Member Resources
- Pathology Case Challenge
- Mediastinum
Clinical Summary
A 60-year-old woman is involved in a motor vehicle accident and is admitted to the emergency department for evaluation of pleuritic chest pain complaints. Rib fractures are noted on chest x-ray. In addition, a 10 cm anterior mediastinal mass is incidentally noted. Fine needle aspiration is performed followed by excision. On resection, the specimen consists of a 10 x 7.5 x 2.5 cm lobulated, firm, and well-defined mass. Cut section reveals a well-circumscribed mass with nodular architecture and without gross evidence of hemorrhage or necrosis.
Master List of Diagnoses
- Follicular dendritic cell tumor/sarcoma
- Nodular sclerosis classical Hodgkin lymphoma
- Primary mediastinal (thymic) large B-cell lymphoma
- Thymic hyperplasia
- Thymoma, type AB
Archive Case and Diagnosis
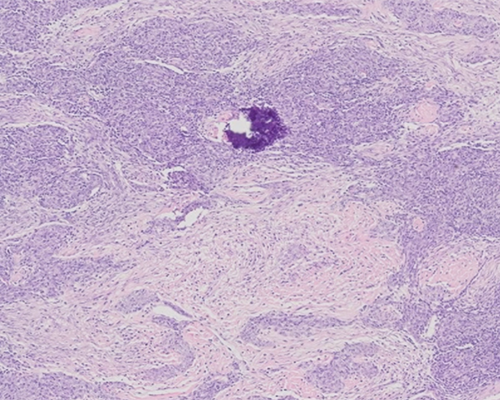
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 22, and is a Thymoma, type AB of the mediastinum.
Criteria for Diagnosis and Comments
The sections show a cellular tumor composed predominantly of bland spindle-shaped epithelial cells with interspersed lymphocytes. Occasional broad fibrous bands are identified. Scattered islands of polygonal epithelial cells are also present. Cystic spaces are noted. Necrosis and mitoses are not identified. More than 10% of the tumor demonstrates a moderate lymphocytic infiltrate. The epithelial component is positive for cytokeratin AE1/AE3. The tumor is well-encapsulated. The clinical presentation and the histologic findings are consistent with a diagnosis of thymoma, type AB.
Thymic epithelial tumors are rare with an approximate incidence of 0.15 cases per 100,000. Thymomas are neoplasms of the thymic epithelial cells and are the most frequent thymic tumor in adults, with a peak incidence between the ages of 55 to 65. Men and women are affected equally. A subset of cases is associated with multiple endocrine neoplasia type 1 syndrome. Thymomas are associated with a variety of autoimmune or paraneoplastic syndromes that may precede the diagnosis of thymoma. Some of the autoimmune disorders are more frequently seen in association with a particular subtype of thymoma. For example, type A thymomas are associated with red cell aplasia and hypogammaglobulinemia. Myasthenia gravis, the most common autoimmune disorder associated with thymoma, is more commonly seen with types B1 and B2. The clinical presentation varies from incidental discovery to complications due to a mediastinal mass resulting in superior vena cava syndrome or respiratory insufficiency.
Stage is still considered the most important prognostic indicator for thymoma. The modified Masaoka staging classification is the one currently accepted and has been shown to be a good predictor of behavior. Stage 1 refers to grossly and microscopically encapsulated thymomas. This includes thymomas that extend into but not through the capsule. Stage 2 tumors either show microscopic transcapsular invasion (stage 2a) or macroscopic invasion into surrounding fatty tissue or grossly adherent to but not through the mediastinal pleura or pericardium (stage 2b). Stage 3 tumors show macroscopic invasion of neighboring structures (ie, pericardium, great vessels, or lung). Stage 4 applies to tumors with hematogenous or lymphatic dissemination.
Historically, the histologic classification of thymomas has been fraught with problems due to overlapping features and the morphologic heterogeneity of the tumors. In 2015 The World Health Organization revised the histologic classification for thymomas. This revised classification provides obligatory and optional criteria for each subtype of thymoma and incorporates immunohistochemistry, creating what is hoped will be more reproducible diagnostic categories. Except for two histologic categories, all thymomas are now considered malignant tumors with the potential to behave aggressively. The exceptions to this are the micronodular and microscopic thymomas.
The classification is based on the tumor epithelial cell morphology, amount of immature T cell (TdT+) lymphocytic infiltrate, and the degree of cytologic atypia. By definition, thymomas do not show overtly malignant cytologic features. If those are present, that indicates thymic carcinoma.
Six subtypes of thymoma exist: A, atypical type A variant, AB, B1, B2, and B3. The atypical type A variant is new. The criteria for each type are as follows:
Revised Morphologic Criteria for Thymoma Classification
Thymoma type |
Obligatory |
Optional |
Type A |
Bland spindle-shaped epithelial cells with minimal TdT+ lymphocytic infiltrate |
Polygonal epithelial cells; CD20 + epithelial cells |
Atypical type A variant |
Same as type A plus comedo-type necrosis, increased mitoses (>4 per 2mm2), nuclear crowding |
Same as type A |
Type AB |
At least focally bland, spindle shaped epithelial cells; numerous immature TdT+ T-cells at least focally or throughout the tumor |
Same as type A |
Type B1 |
Bland epithelial polygonal or dendritic tumor cells, a prominent immature lymphocytic infiltrate, and evidence of medullary differentiation (medullary islands). There is no evidence of clustering (defined as <3 contiguous epithelial cells) |
Hassall corpuscles; perivascular spaces |
Type B2 |
Increased clustering of polygonal or dendritic epithelial cells and numerous infiltrating (TdT+) T lymphocytes |
Same as type B1 plus medullary islands |
Type B3 |
Sheets of mild to moderately atypical epithelial cells with absent to minimal TdT+ lymphocytic component |
Same as B1 |
Micronodular Thymoma |
Nodules of bland spindle or oval epithelial cells surrounded by a lymphoid stroma |
Lymphoid follicles; monoclonal B cells and/or plasma cells |
Metaplastic Thymoma |
Biphasic tumor composed of solid areas of epithelial cells in a background of bland-looking spindle cells; absence of immature T cells |
Pleomorphism of epithelial cells; actin, keratin, or EMA-positive spindle cells |
Adapted from Marx A, Chan JKC, Coindre, JM, et al. The 2015 World Health Organization classification of tumors of the thymus: continuity and changes. J Thorac Oncol. 2015;10:1383-1395.
More than 30% of thymomas can show more than one histologic type. Therefore, it is currently recommended that all the histologic types identified be reported with the most common morphology first and subsequent morphologies included and quantified in 10% increments.
Special categories of thymoma include micronodular thymoma composed of nodules of bland spindle or oval epithelial cells surrounded by a lymphoid stroma lacking epithelial cells, combined thymoma referring to thymomas containing a carcinoma component, and metaplastic thymoma, a biphasic tumor with solid areas of epithelial cells in a background of bland-looking spindle cells without lymphocytes. Thymic carcinoma is a malignant tumor with overt cytologic atypia.
Immunostains can aid in the diagnosis of thymoma and in its subclassification. The epithelial cells of normal thymus, thymoma, and thymic carcinoma are positive for cytokeratin 19, p40, PAX-8, and p63. The epithelial cells of thymic carcinoma are distinguished by their expression of CD117 and CD5. The epithelial cells of Type A and Type AB thymomas may express CD20, a potential pitfall in the differentiation from lymphoma. The immature T-cells of normal thymus are positive for TdT and CD5.
The differential diagnosis of thymoma includes thymic hyperplasia, classic Hodgkin lymphoma, primary mediastinal (thymic) large B-cell lymphoma, and follicular dendritic cell tumor/sarcoma. Thymic hyperplasia can be difficult to separate from type B1 thymoma. Type B1 thymoma is the subtype that most closely resembles normal thymus and can have Hassall corpuscles and medullary islands. A prominent fibrous capsule and a greater component of cortical areas over medullary areas favor a type B1 thymoma.
Primary mediastinal (thymic) large B-cell lymphoma (PMBCL) is a subtype of diffuse large B-cell lymphoma arising in the mediastinum that is thought to be of thymic origin. It primarily affects young adults between the ages of 30 to 40 with a 1:2 male to female ratio. Histologically, the tumor is composed of atypical medium to large lymphoid cells in a sclerotic background. The sclerosis often wraps around the atypical lymphoid cells creating a pseudoalveolar-like pattern, so called compartmentalizing alveolar fibrosis. The tumor cells have irregular nuclear borders and sometimes prominent eosinophilic nucleoli resembling Reed-Sternberg cells. Multilobated cells may be present. Residual thymic tissue may be present, but Hassall corpuscles are usually not found. Differentiation from thymoma is not usually a problem unless there is extensive fibrosis or sclerosis. This can cause confusion with the sclerotic form of thymoma. Immunohistochemistry can assist in separating thymoma and PMBCL. PMBCL is positive for C20, CD79a, PAX5, and often dim CD30. p63 can also be positive and needs to be interpreted in the context of other stains as p63 also stains normal and neoplastic thymic epithelial cells.
Nodular sclerosis classic Hodgkin lymphoma (NSHD) involves the mediastinum in 80% of cases. Grossly, the tumors are firm, white, and nodular. Microscopically, there are broad fibrous bands and characteristic Reed-Sternberg cells. Retraction artifact is often present around some of these, giving the cells the appearance of being in clear lakes, thus the name lacunar cells. NSHD can be differentiated from thymoma by the mixed inflammatory cell infiltrate, Reed-Sternberg cells that express CD30 and CD15 but not CD45, and EBER positivity in a subset of cases, and the lack of a TdT positive population. Cytokeratin stains are negative in NSHD and positive in thymoma.
Follicular dendritic cell tumor/sarcoma (FDCS) is a rare neoplastic proliferation of neoplastic follicular dendritic cells that usually occurs in lymph nodes but can occur extranodally including the mediastinum. The tumors can have a nodular appearance grossly. The tumor cells are ovoid to spindled mimicking the cells of a type A or AB thymoma. Interdigitating lymphocytes can be present. Immunohistochemistry is very useful as FDCS cells express CD23 and CD21. Cytokeratin and p63 are usually negative in FDCS. Hassall corpuscles are absent in FDCS and their presence would favor thymoma.
Supplementary Questions
- A 50-year-old woman with myasthenia gravis presents with a mediastinal mass and pleural metastases. A diagnosis of thymoma is made following biopsy. Which of the following features is the most important in assessing prognosis?
- Histologic type
- Mitotic activity
- Necrosis
- Nodular growth pattern
- Stage
- A 40-year-old woman presents with dyspnea and a mediastinal mass. A fine needle aspiration is performed and shows spindled to oval bland cells with background lymphocytes. Based on the findings which of the following is correct?
- CD20, CD79a, and CD30 stains would be a useful panel in this setting.
- CD21, CD23, and cytokeratin stains would be a useful panel to exclude follicular dendritic cell tumor/sarcoma.
- CD30, CD15, and EBV stains would be helpful as these morphologic findings are suggestive of primary mediastinal large B-cell lymphoma.
- The findings are most consistent with benign thymic tissue. No further evaluation is needed.
- These features are diagnostic of thymoma type AB.
- A 50-year-old woman with myasthenia gravis is noted to have an enlarged thymus. A thymectomy is performed. The sections show clusters of polygonal epithelial cells with intermingled TdT+ lymphocytes. This histologic pattern is most characteristic of which of the following diagnoses?
- Thymic hyperplasia
- Type A thymoma
- Type AB thymoma
- Type B1 thymoma
- Type B2 thymoma
References
- den Bakker MA, Roden AC, Marx A, Marino M. Histologic classification of thymoma: A practical guide for routine cases. J Thoracic Oncol. 2014;9(9):S125-S130.
- Green AC, Marx A, Strobel P, et al. Type A and AB thymomas: histological features associated with increased stage. Histopathology. 2015;66:884-891.
- Hartert M, Strobel P, Dahm M, et al. A follicular dendritic cell sarcoma of the mediastinum with immature T cells and association with myasthenia gravis. Am J Surg Pathol 2010;34(5):742-745.
- Marx A, Chan JKC, Coindre J-M, et al. The 2015 World Health Organization classification of tumors of the thymus: continuity and changes. J Thorac Oncol. 2015;10:1383-1395.
- Travis WD, Brambilla E, Burke AP, Nicholson AG. 2015 WHO Classification of Tumors of the Lung, Pleura, Thymus and Heart. 4th ed. Lyon, FR: International Agency for Research on Cancer; 183-287.
- Wang H, Sima CS, Beasley MB, et al. Classification of thymic epithelial neoplasms is still a challenge to thoracic pathologists: a reproducibility study using digital microscopy. Arch Pathol Lab Med. 2014; 138:658-663.
Author
Deborah Ann Belchis, MD
Surgical Pathology Committee
Johns Hopkins Bayview Medical Center
Baltimore, MD
Answer Key
- Stage (e)
- CD21, CD23, and cytokeratin stains would be a useful panel to exclude follicular dendritic cell tumor/sarcoma. (b)
- Type B2 thymoma (e)