Clinical Summary
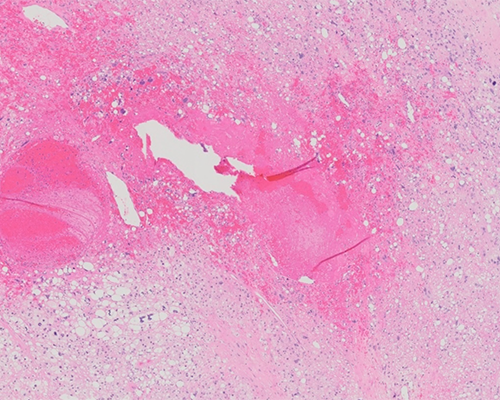
An 81-year-old man presents with a 9.0 cm intramuscular neck mass. Gross examination reveals a soft, yellow to gray-white, well-delineated, non-encapsulated, focally hemorrhagic tumor encased in red-brown skeletal muscle.
Master List of Diagnoses
- Dedifferentiated liposarcoma, metastatic
- Pleomorphic liposarcoma
- Pleomorphic rhabdomyosarcoma
- Pseudolipoblastic melanoma
- Undifferentiated pleomorphic sarcoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 04, and is pleomorphic liposarcoma of the neck.
Criteria for Diagnosis and Comments
Histologic examination reveals a tumor composed of markedly atypical round to spindle cells with atypical mitotic activity and necrosis, punctuated by several large, bizarre lipoblasts, characterized by multiple cytoplasmic vacuoles scalloping hyperchromatic enlarged nuclei. These features are diagnostic for pleomorphic liposarcoma.
Pleomorphic liposarcoma is a high-grade, biologically-aggressive sarcoma with 30% to 50% risk for metastatic potential and 40% to 50% associated mortality. The majority of pleomorphic liposarcomas arise in elderly patients (greater than 50 years) with an equal sex distribution. While these tumors can occur in the superficial dermis, these more commonly involve deep, intramuscular locations. Most common anatomic locations for pleomorphic liposarcoma include the extremities (lower > upper limbs), with the trunk and the retroperitoneum being less frequent sites. Rarely the mediastinum, paratesticular region, scalp/neck, abdominal/pelvic cavities, and even orbit may be affected. Lung is the most common site for metastasis. The behavior for this pleomorphic adipocytic-phenotype tumor, however, is not as poor as for other pleomorphic sarcomas, including myoid pleomorphic sarcomas (pleomorphic leiomyosarcoma and pleomorphic rhabdomyosarcoma) and angiosarcoma.
Pleomorphic liposarcoma is a high-grade pleomorphic sarcoma demonstrating a variable number of pleomorphic lipoblasts. The epithelioid variant of pleomorphic liposarcoma is characterized by sheets of mostly univacuolated to multivacuolated lipoblasts, without intervening spindled and pleomorphic areas. By immunohistochemistry, pleomorphic liposarcoma can demonstrate S100 protein positivity in the bizarre lipoblasts and CD34 positivity in spindled areas. The epithelioid variant of pleomorphic liposarcoma can be keratin positive. MIB-1 would be expected to have a high index in all pleomorphic sarcomas; mitoses may be further apart (resulting in fewer per 10 high-power fields[HPF]) in tumors with large, bizarre nuclei or lipoblasts due to large size of tumor cells.
Pleomorphic liposarcoma represents the rarest subtype of liposarcoma, accounting for less than 5% of all liposarcomas and 20% of pleomorphic sarcomas overall. In general, liposarcomas can be classified into 3 main groups: (1) well-differentiated and dedifferentiated liposarcomas, which share genetic findings of MDM2 and changes in chromosome 12q13-15 with ring chromosome, (2) myxoid and round cell liposarcomas, which share a common t(12:16)(q13;p11) translocation involving DDIT3 (CHOP) and FUS or less commonly EWSR1, and (3) pleomorphic liposarcoma and its epithelioid variant, which often has a complex karyotype but does not show amplification of MDM2.
The differential diagnosis for pleomorphic liposarcoma includes dedifferentiated liposarcoma, pleomorphic rhabdomyosarcoma, undifferentiated pleomorphic sarcoma, and pseudolipoblastic melanoma.
Dedifferentiated liposarcoma most commonly occurs in the retroperitoneum and typically shows a transition from well-differentiated liposarcoma to a non-lipogenic sarcoma. Well-differentiated liposarcoma shows adipocytic areas with widened fibrous septa and atypical stromal cells, rather than bizarre lipoblasts. Dedifferentiated areas may show low-grade or high-grade morphology, and most frequently show features similar to undifferentiated pleomorphic sarcoma or myxofibrosarcoma. Expression of MDM2 by immunohistochemistry or identification of MDM2 amplification is helpful to distinguish this tumor from pleomorphic liposarcoma.
Pleomorphic rhabdomyosarcoma is a high-grade sarcoma demonstrating sheets of large atypical round to spindle cells, often with abundant eosinophilic cytoplasm. Instead of the lipoblasts seen in pleomorphic liposarcoma, these tumors demonstrate skeletal muscle differentiation and often show strong desmin expression and variably express myoD1 and myogenin by immunohistochemistry.
Undifferentiated pleomorphic sarcoma is a subtype of undifferentiated soft tissue sarcoma, a group of mesenchymal neoplasms that lack an identifiable line of differentiation. Histologically, these tumors are composed of spindle and pleomorphic cells with atypical mitoses and frequent bizarre, multinucleated cells. Unlike pleomorphic liposarcoma, lipoblasts will be absent.
Pseudolipoblastic melanoma is a rare morphologic variant of melanoma characterized by the presence of intracytoplasmic vacuoles with nuclear scalloping, imparting a pseudolipoblastic appearance. This tumor would express melanocytic markers, including HMB45, Melan-A, Mitf, and Tyrosinase.
Supplementary Questions
- Which of the following criteria can be used to diagnose “pleomorphic liposarcoma” and separate it from “dedifferentiated liposarcoma”?
- Anatomic location
- MDM2 positivity
- Patient age
- Presence of bizarre lipoblasts
- Tumor depth
- Which of the following molecular findings supports a diagnosis of myxoid liposarcoma?
- DDIT3 (CHOP) amplification
- DDIT3 (CHOP) translocation
- EWS rearrangement
- MDM2 amplification
- MDM2 translocation
- Which of the following immunostains would all be positive in epithelioid variant of pleomorphic liposarcoma?
- Keratin, CD20, CEA, and NSE
- Keratin, NSE, Melan-A, and chromogranin
- Keratin, S100, CD34, and MIB-1
- S100, CD34, MDM2, and CD31
- S100, Melan-A, BRAF, and HMB45
References
- Anderson WJ, Jo VY. Pleomorphic liposarcoma: updates and current differential diagnosis. Semin Diagn Pathol. 2019;36:122-128.
- Banerjee SS, Harris M. Morphological and immunophenotypic variations in malignant melanoma. Histopathology. 2000;36:387-402.
- Demicco EG. Molecular updates in adipocytic neoplasms. Semin Diagn Pathol. 2019;36:85-94.
- Fanburg-Smith JC, Furlong MA, Childers ELB. Liposarcoma of the oral and salivary gland region. A clinicopathologic study of 18 cases with emphasis on specific sites, morphologic subtypes and clinical outcome. Mod Pathol. 2002;15(10):1020-1031.
- Fanburg-Smith JC, Miettinen M. Liposarcoma with meningothelial-like whorls: a study of 17 cases of a distinctive histologic pattern associated with dedifferentiated liposarcoma. Histopathology. 1998;33:414-424.
- Lasota J, Marwaha J, Fanburg-Smith JC. CHOP is Not Rearranged in Epithelioid Pleomorphic Liposarcoma: Fluorescence in Situ Hybridization (FISH) Study on Four Cases. Mod Pathol. 2009:2(1):17A.
- Miettinen M, Enzinger FM. Epithelioid variant of pleomorphic liposarcoma: a study of 12 cases of a distinctive variant of high-grade liposarcoma. Mod Pathol. 1999;12(7):722-728.
- Murphey MD, Arcara LK, Fanburg-Smith JC. From the archives of the AFIP: imaging of musculoskeletal liposarcoma with radiologic-pathologic correlation Radiographics. 2005; 25:1371-1395.
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours of Soft Tissue and Bone Tumours. 5th ed. IARC Press; 2020.
Author
Julie C. Fanburg-Smith, MD, FCAP
Surgical Pathology Committee
Penn State Health/Milton S. Hershey Medical Center
Hershey, PA
Answer Key
- Presence of bizarre lipoblasts (d)
- DDIT3 (CHOP) translocation (b)
- Keratin, S100, CD34, and MIB-1 (c)