- Home
- Member Resources
- Pathology Case Challenge
- Pancreas
Clinical Summary
A 62-year-old woman presents with abdominal pain and nausea. A computed tomography (CT) scan shows a well-circumscribed, multilocular mass with a prominent central scar in the tail of the pancreas. No masses are noted outside of the pancreas.
Master List of Diagnoses
- Intraductal papillary mucinous neoplasm
- Mucinous cystadenoma
- Pancreatic pseudocyst
- Serous cystadenocarcinoma
- Serous cystadenoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 01, and is serous cystadenoma of the pancreas.
Criteria for Diagnosis and Comments
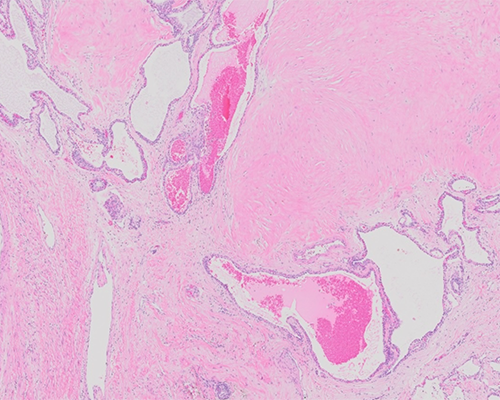
Sections show a tumor composed of multiple cysts of various size lined by a single layer of cuboidal or flattened simple epithelium. The cells have eosinophilic to clear cytoplasm with well-defined cytoplasmic borders. The nucleus is round, uniform, and centrally located. Areas of necrosis, nuclear atypia, and mitotic figures are not noted. A prominent capillary network is present adjacent to the cysts. These features are consistent with a diagnosis of serous cystadenoma (SCA).
SCA is a benign pancreatic neoplasm, accounting for 1% - 2% of all pancreatic neoplasms. It has a marked female predominance (female to male ratio as high as 3 - 7 to 1) and a mean age at presentation around 65 years (range 18 - 91). SCAs can occur anywhere in the pancreas but show a slight predilection for the body and tail. About one-third of patients are asymptomatic and the tumor is discovered incidentally, while two-thirds of patients present with abdominal pain, abdominal mass, nausea, vomiting, or weight loss. Jaundice is an uncommon presenting symptom. There is an association with von Hippel-Lindau (VHL) syndrome; up to 90% of VHL patients develop pancreatic SCAs.
The best imaging modalities for SCA are ultrasound and contrast-enhanced CT, which show a well-defined tumor composed of microlacunae, separated by delicate septae with a central stellate scar. On T1-weighted magnetic resonance imaging (MRI) SCAs are hypointense while on T2-weighted MRI they are hyperintense due to the fluid content. There is no communication between the cysts of SCA and the pancreatic ductal system.
On macroscopic examination, SCAs show a well-defined, slightly bosselated tumor with a mean size of 6.0 cm (range from 1 to 25 cm). On cross section, SCAs have a sponge-like appearance imparted by numerous small cysts filled with serous fluid. A central scar is often observed and may show calcifications.
Microscopic examination reveals a microcystic architecture with numerous cysts lined by cuboidal cells with clear/pale to eosinophilic cytoplasm. Occasional micropapillary projections may be seen. The cells contain intracytoplasmic glycogen and as a result are positive for PAS without diastase digestion and negative for PAS-diastase. The cells of SCA express cytokeratin, alpha-inhibin, MUC6, and in about 1/3 of cases MUC1.
Between 40% - 70% of sporadic SCAs show loss of heterozygosity and/or inactivating mutations of the VHL gene. There are no mutations identified in KRAS and TP53 genes, which are commonly affected in usual ductal adenocarcinoma of the pancreas.
There are several histologic variants of SCA described in addition to the usual microcystic pattern including macrocystic serous cystadenoma, solid serous cystadenoma, VHL-associated serous cystic neoplasm, and mixed serous neuroendocrine neoplasm. Macrocystic serous cystadenoma is composed of few large cysts or may be unilocular. It usually involves the head of the pancreas and often lacks a central scar. Solid serous adenoma is composed of tumor cells arranged in small acini, sheets, or trabeculae with inconspicuous central lumina. The cytological features and immunohistochemical profile are similar to regular SCAs; however, this variant is usually characterized by a smaller size. VHL-associated serous cystic neoplasms have an identical histology to sporadic SCAs; however, they tend to involve the pancreas diffusely or patchily without a distinct mass. The mixed serous neuroendocrine neoplasm is a rare variant in which an SCA is associated with a pancreatic endocrine neoplasm that can be separate or admixed with the cystic structures. This variant is also often associated with VHL syndrome.
Treatment of SCA involves complete resection, which is usually curative. Conservative managements can be considered for small lesions with typical morphology on imaging studies.
The clinical presentation, gross examination, and histology of SCA are highly characteristic and therefore positive diagnosis is usually straightforward. Differential diagnosis includes other pancreatic cystic tumors such as mucinous cystadenoma or intraductal papillary mucinous neoplasm, reactive conditions characterized by cysts including pancreatic pseudocyst and serous cystadenocarcinoma.
Mucinous cystadenomas almost always arise in women and in the tail of the pancreas. They are composed of multilocular, thick-walled cysts lined by mucinous epithelium with variable degree of atypia. The cysts are surrounded by a characteristic band of ovarian-type stroma composed of spindle cells with scant cytoplasm and wavy nuclei.
Intraductal papillary mucinous neoplasms (IPMNs) account for about 20% of cystic pancreatic lesions. They are most commonly encountered in the pancreatic head and present with a markedly dilated main pancreatic duct with papillary projections (in the main-duct or combined type) or with single or multiple peripheral cysts that connect with the main duct (in the branch-duct type). As opposed to SCA, IPMNs do not form a well-defined mass.
Pancreatic pseudocysts are the most common type of pancreatic cystic lesions. They present as a unilocular cyst with a thick fibrous wall. On histologic examination, the wall is composed of granulation tissue and fibrosis without an epithelial lining. Extensive sampling is recommended to document absence of an epithelial lining.
Serous cystadenocarcinoma is a very rare tumor that is morphologically indistinguishable from SCA. As opposed to SCA, serous cystadenocarcinoma is larger and shows extrapancreatic extension with direct invasion into adjacent structures or spread to lymph nodes, spleen, stomach, duodenum, liver, and peritoneum.
Supplementary Questions
- Which of the following gross and/or histologic features is characteristic of serous cystadenoma?
- Dilatation of main pancreatic duct with papillary projections
- Extrapancreatic extension
- Multilocular thick-walled cysts lined by mucinous epithelium
- Unilocular cyst with a thick fibrous wall
- Well-circumscribed tumor with sponge-like appearance
- Which of the following syndromes is associated with serous cystadenoma?
- Birt-Hogg-Dube
- Cowden
- Familial pancreatic cancer
- Muir-Torre
- Von Hippel-Lindau
- Which of the following genes is commonly affected in usual ductal adenocarcinoma of the pancreas?
- CTNNB
- KRAS
- MITF
- NF1
- VHL
References
- Terris B, Fukushima N, Hruban RH. Serous neoplasms of the pancreas. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. WHO Classification of Tumours of the Digestive System. IARC. 2010;296-299.
- Kim GE. Serous cystadenoma. In: Lamps LW, eds. Diagnostic pathology hepatobiliary and pancreatic, Amirsys. 2011;II5:14-17.
- Chu LC, Singhi AD, Haroun RR, Hruban RH, Fishman EK. The many faces of pancreatic serous cystadenoma: Radiologic and pathologic correlation. Diagn Interv Imaging. 2017;98(3):191-202.
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumors: Digestive System Tumours. 5th ed. IARC; 2019.
Author
Aleodor A. Andea, MD, MBA
Surgical Pathology Committee
University of Michigan
Ann Arbor, MI
Answer Key
- Well-circumscribed tumor with sponge-like appearance (e)
- Von Hippel-Lindau (e)
- KRAS (b)