Clinical Summary
A 30-year-old man status post chemotherapy and left orchiectomy for a testicular tumor presents with a left scrotal mass, which is resected. Serum alpha-fetoprotein, hCG, and LDH levels are elevated. On resection, the 10 cm nodular mass has a variegated appearance with hemorrhage and necrosis. A subset of cells are CD30 and OCT3/4 positive and another subset stains with alpha fetoprotein (AFP) and glypican 3.
Master List of Diagnoses
- Choriocarcinoma
- Embryonal carcinoma
- Mixed germ cell tumor
- Seminoma
- Teratoma, post-pubertal type
- Yolk sac tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 21, and is seminoma in the testis.
The information provided in this case was accurate and correct at the time of publication in 2020. Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
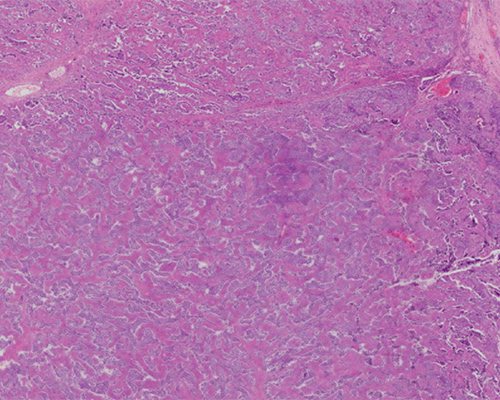
Microscopically, the tumor is composed of sheets of uniform, polyhedral cells within vague lobules separated by eosinophilic, fibrous septae laden with lymphocytes. The polyhedral cells contain glycogen that causes the cytoplasm to appear glassy/clear when stained with hematoxylin and eosin (H&E). The cells have distinct cell borders with nonmolding, nonoverlapping, large, and centrally located nuclei with prominent nucleoli, giving them a low nucleus:cytoplasm (N:C) ratio when compared to the interspersed lymphocytic infiltrate. This appearance demonstrates the features of a seminoma.
Seminomas are the most common testicular germ cell neoplasms encountered in men 15 to 44 years of age, with a median age of 37 to 41 and a 5:1 predominance in white vs. black males. Pure seminomas comprise 50% of all testicular germ cell tumors, with 17% of the remaining germ cell neoplasms containing a seminomatous component (mixed germ cell tumors). Nonseminomatous germ cell tumors include choriocarcinomas, embryonal carcinomas, yolk sac tumors, teratoma, and spermatocytic tumors (formerly known as spermatocytic seminomas).
Clinically, seminomas typically present as painless unilateral testicular masses. Two percent of seminomas present bilaterally, and less than 5% present with spermatic cord involvement. On gross examination, testes with seminomas will manifest as homogeneous, solid tan to cream to yellow fleshy nodules, potentially with circumscribed necrotic areas. Hemorrhagic or cystic areas may suggest the presence of another germ cell tumor type. Because seminoma cells are not cohesive, they tend to be smeared easily when manipulating the specimen; it is recommended to collect margins before cutting into the tumor. Positive margins will most likely be evident grossly.
10% to 20% of all seminomatous tumors contain syncytiotrophoblasts. When present, these large, multinucleated cells are responsible for producing β-hCG, which is detectable in the patient’s serum. These tumors are diagnosed as “seminomas with syncytiotrophoblastic cells.” Granulomatous reactions also occur.
Immunohistochemical (IHC) staining indirectly illustrates genetic abnormalities retained by seminoma cells. Seminomas with nuclear localization of octamer binding transcription 4 (OCT3/4) and homeobox protein NANOG (named in honor of the Irish “Tír na nÓg,” land of eternal youth) have defects of isochromosome 12p. Positive IHC nuclear staining of NANOG and OCT3/4 is not specific; dysgerminomas (the ovarian counterpart of seminomas in females) and some embryonal carcinomas that contain isochromosome 12p will stain positive for NANOG and OCT3/4 as well.
Seminomas show cytoplasmic and membranous staining for placental alkaline phosphatase (PLAP) and podoplanin (D2-40), and nuclear staining for the transcription factor Spalt-like protein 4 (SALL4). If syncytiotrophoblasts are present, their cytoplasm will stain positive for β-hCG. Seminoma cells stain positively for the receptor tyrosine kinase KIT (CD117). CD117 immunoreactivity does not correlate with an activating KIT mutation: virtually all seminomas mark with CD117, but only 25% possess the activating gene mutation.
Diagnostic laboratory testing can be helpful for confirming a diagnosis of seminoma. In spite of being nonspecific, serum LDH correlates with tumor burden. β-hCG positivity in the serum of a male with a testicular tumor may indicate that the tumor has syncytiotrophoblastic cells present. If AFP is elevated, the tumor is more than likely a mixed germ cell tumor with a yolk sac tumor component.
The histologic morphology is often sufficient to diagnose a seminoma, but IHC may be needed to help rule out similar tumors. Other tumors that resemble seminomas in morphology include embryonal carcinomas, solid yolk sac tumors, spermatocytic tumors, lymphoma and metastatic carcinoma.
Metastatic carcinomas, like metastatic prostate adenocarcinoma, and lymphomas, like diffuse large B-cell lymphoma, can occasionally be in the differential diagnosis. A panel of IHC stains specific for carcinoma (AE1/AE3, PSA, NKX3.1) or lymphoma (CD45) should quickly help with differentiation.
Embryonal carcinoma, the second most prevalent testicular germ cell neoplasm, can have a similar appearance to seminoma grossly. Classic embryonal carcinoma cells are large with pleomorphic, vesicular nuclei containing macronucleoli, poorly defined membranes and amphophilic cytoplasm. There are usually numerous mitotic figures and apoptotic bodies. Some of the cells can have well-defined cytoplasmic membranes and cleared-out cytoplasm, resembling seminoma cells. IHC staining of embryonal carcinomas includes positivity for CD30, SOX2 and cytokeratins but negative staining for KIT and SOX17. Seminomas, on the other hand, stain positive for KIT and SOX17 and are negative for CD30, SOX2, and the majority of tumor cells are negative for cytokeratin. OCT3/4 stains positively in both seminomas and embryonal carcinomas, and thus cannot be used to differentiate the two (like seminomas, some embryonal carcinomas will also harbor an isochromosome 12p).
Pure yolk sac tumors are much less common than seminomas, comprising 0.6% of testicular germ cell neoplasms. Yolk sac tumors are more commonly found as components within a mixed germ cell tumor, occurring in 44% of nonseminomatous germ cell tumors in patients 15 to 40 years of age. Solid-pattern yolk sac tumors are composed of cohesive, polygonal cells with clear to eosinophilic cytoplasm and well-defined cell borders and can resemble seminoma, but the yolk sac tumor typically lacks lymphocytes or fibrous septae. Yolk sac tumors stain positive with glypican3 and AFP, are strongly positive for AE1/AE3 (cytokeratin) and are negative for OCT3/4; seminomas stain positive for OCT3/4, are generally negative for AE1/AE3 and do not stain with AFP.
Spermatocytic tumors, formerly known as spermatocytic seminomas, are triphasic tumors that contain cells similar to seminoma cells – large giant cells (which can be multinucleated), intermediate-size cells with spireme nuclei (lacy chromatin akin to the shape of a spider) and eosinophilic cytoplasm, and small cells with a high N:C ratio and dark nuclei. Spermatocytic tumors have distinct IHC staining patterns that separate them from seminomas – spermatocytic tumors stain negatively for NANOG, OCT3/4, PLAP, and D240 (all of which stain positively in seminomas). Spermatocytic tumors also do not have an isochromosome 12p.
| Seminoma | Embryonal Carcinoma | Yolk Sac Tumor | Spermatocytic Tumor |
D2-40 | (+) CP/M | (-) | (-) | (-) |
CD117 | (+) CP/M | (-) | (+) CP/M | (+) CP/M |
SOX17 | (+) N | (-) | (-) | U |
SOX2 | (-) | (+) N | (-) | U |
CD30 | (-) | (+) M | (-) | (-) |
AE1/AE3 | (-) | (+) CP/M | (+) CP/M | (-) |
NANOG | (+) N | (+) N | (-) | (-) |
OCT3/4 | (+) N | (+) N | (-) | (-) |
Glypican3 | (-) | (-) | (+) CP/M | U |
AFP | (-) | (-) | (+) CP | (-) |
PLAP | (+) CP/M | (-); rare patchy | (+) CP/M | (-) |
SALL4 | (+) N | (+) N | (+) N | (+) N |
βhCG | (-)/(+) in CP of syncytiotrophoblasts | (-) | (-) | (-) |
N: Nuclear staining, CP: Cytoplasmic staining, M: Membranous staining, U: Unknown/no data
Supplementary Questions
- Which of the following is true regarding seminomas?
- A normal serum AFP rules out the diagnosis of a seminoma.
- Both seminomas and embryonal carcinomas may contain an isochromosome 12p.
- Seminomas contain medium-sized diploid cells with spireme nuclei.
- Seminomas typically present with bilateral palpable testicular nodules.
- The majority of seminomas produce beta-human chorionic gonadotropin.
- Which of the following serum analytes has the most clinical utility in distinguishing pure seminomas from mixed germ cell tumors?
- AFP
- β-hCG
- CEA
- LDH
- PLAP
- IHC staining of which of the following will help differentiate a seminoma from an embryonal carcinoma?
- CD30
- NANOG
- OCT3/4
- β-hCG
- SALL4
References
- Amin MB, Edge SB, Greene FL, et al, eds. AJCC Cancer Staging Manual. 8th ed. Springer International Publishing; 2017:735-743.
- Aparicio J, Terrasa J, Durán I, et al. SEOM clinical guidelines for the management of germ cell testicular cancer (2016). Clin Transl Oncol. 2016;18(12):1187-1196.
- Cavaleri F, Schöler HR. Nanog: a new recruit to the embryonic stem cell orchestra. Cell. 2003;113(5):551-552.
- Chen Y, Qi C, Xia L, Li G. Identification of novel genetic etiology and key molecular pathways for seminoma via network-based studies. Int J Oncol. 2017;51(4):1280-1290.
- Dieckmann KP, Simonsen-Richter H, Kulejewski M, et al. Serum tumour markers in testicular germ cell tumours: frequencies of elevated levels and extents of marker elevation are significantly associated with clinical parameters and with response to treatment. BioMed Res Int. 2019;2019:1-22.
- IrishCentral.com. Tír Na nÓg - The legend of the land of eternal youth. Accessed August 11, 2019. https://www.irishcentral.com/r...
- Lester SC. Manual of Surgical Pathology. 3rd ed. Elsevier Saunders; 2010;406-413.
- Moch H, Humphrey PA, Ulbright TM, Reuter VE, eds. WHO Classification of Tumours of the Urinary System and Male Genital Organs. 4th ed. IARC; 2016;185-221.
Answer Key
- Both seminomas and embryonal carcinomas may contain an isochromosome 12p. (b)
- AFP (a)
- CD30 (a)