Clinical Summary
A 45-year-old woman presents to her internist with fatigue, constipation, dry skin, weight gain, and mild difficulty in swallowing over the past few months. On physical examination, she has facial edema which is prominent periorbitally. Her skin is dry, and her hands and feet show mild nonpitting edema. Her serum shows elevated anti-thyroglobulin and antithyroid peroxidase (anti-TPO) antibodies. Her thyroid gland is enlarged, firm, and rubbery, without tenderness or bruit.
She undergoes total thyroidectomy, which reveals a clearly demarcated capsule that is non-adherent to the surrounding structures. The thyroid gland weighs 25 grams, and, on sectioning, shows a white cut surface with a “fish flesh” appearance, but no distinct nodules.
Master List of Diagnoses
- Hashimoto thyroiditis
- Hürthle cell adenoma
- Hürthle cell carcinoma
- Mucosa associated lymphoid tissue lymphoma
- Papillary thyroid carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 37, and is Hashimoto thyroiditis.
Criteria for Diagnosis and Comments
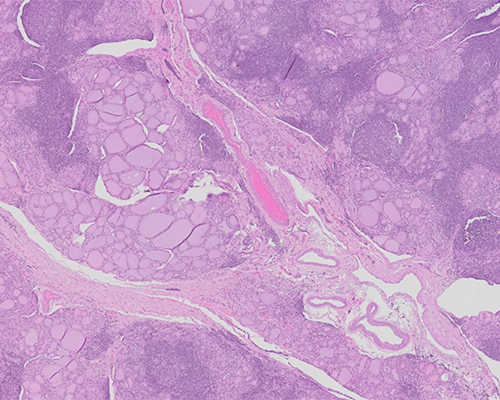
Microscopic sections from the thyroid gland show extensive lymphocytic infiltrate with formation of germinal centers in some areas. There are atrophic follicles with abundant Hürthle cells/oncocytes intermixed with scattered areas of fibrosis and giant cell reaction limited to the thyroid parenchyma. Some of the nuclei are enlarged and overlapping with partial nuclear clearing, but without any intranuclear inclusions. There are areas with large squamous nests, and focal areas show hyperplastic lymphoid follicles. By immunostains, the lymphocytes are predominantly T cells, and plasma cells are polyclonal, expressing both kappa and lambda light chains. The overall histologic features are supportive of Hashimoto thyroiditis.
Hashimoto thyroiditis, also known as chronic lymphocytic thyroiditis or struma lymphomatosa, was first described by Hakaru Hashimoto. It is primarily a disease of adult women, with a female-to-male ratio of approximately 7:1, but can also occur in children. It is the most common cause of hypothyroidism in iodine-sufficient areas of the world. Thyroid failure is seen in up to 10% of patients with Hashimoto thyroiditis and its prevalence increases with age. It is now recognized as an autoimmune thyroid disease and is characterized by high titers of circulating antibodies to thyroid peroxidase and thyroglobulin. The cause of Hashimoto thyroiditis is thought to be a combination of genetic susceptibility and environmental factors. On microscopic examination of the thyroid gland, there is dense lymphoplasmacytic infiltration and lymphoid follicle formation with well-developed germinal centers. Hürthle cell (oncocytic) change is often seen in follicular epithelium.
However, Hashimoto thyroiditis is not a histopathologically homogeneous lesion, and several subtypes of Hashimoto thyroiditis, which present with clinicopathological features that are quite distinct from typical Hashimoto thyroiditis, have been described. The most recognized subtype is the fibrous variant of Hashimoto thyroiditis, which is characterized by marked fibrous replacement of the thyroid parenchyma and microscopic changes typical of Hashimoto thyroiditis in the remaining tissue. In contrast to Riedel thyroiditis, there is no extrathyroidal fibrosis in the fibrous variant of Hashimoto thyroiditis. Some of the patients with this variant of Hashimoto thyroiditis may have IgG4 thyroiditis and show a predominant interfollicular pattern of fibrosis, along with increased IgG4-positive plasma cells and increased serum IgG. These patients are often treated with thyroid hormone replacement, surgery being indicated in certain conditions. Most patients have an excellent prognosis.
Hürthle cell neoplasms of the thyroid show a distinct nodule or nodules that are comprised mostly of large oncocytes with distinct cell borders, deeply eosinophilic and granular cytoplasm, and a large nucleus with prominent nucleolus. On ultrastructural examination, the oncocytes typically show abundant mitochondria. These neoplasms can show follicular, trabecular, solid, or papillary growth patterns with occasional nuclear grooves or nuclear pseudoinclusions. However, these neoplasms have a distinct nodular appearance without abundant lymphocytes and plasma cells typically seen in Hashimoto thyroiditis. The distinction between Hürthle cell adenoma and carcinoma is based on presence of capsular or vascular invasion, or both.
Preexisting Hashimoto thyroiditis is the only known risk factor for primary mucosa associated lymphoid tissue (MALT) lymphoma. Approximately one-half of patients with MALT lymphoma have Hashimoto thyroiditis. Among patients with Hashimoto thyroiditis, the risk of thyroid lymphoma is at least 60 times higher than in patients without thyroiditis. It is important to perform immunostains if the histological features are suspicious for lymphoma, to prove that the lymphocytes are predominately of T cell type and the plasma cells are polyclonal.
MALT lymphoma of thyroid gland shows infiltration of thyroid epithelium by the neoplastic lymphocytes and formation of lymphoepithelial lesions. Some patients with MALT lymphoma may have background lymphocytic thyroiditis and may be misdiagnosed with lymphocytic thyroiditis. MALT lymphoma is characterized by the presence of atypical lymphoid cells, which originate within the marginal zone of the lymphoid follicles and can extend into the interfollicular space, germinal centers (follicular colonization), or both. The diagnosis of lymphoma is supported by the presence of a dense clonal proliferation of monotonous lymphoid cells and the presence of lymphoepithelial lesions. MALT lymphomas express B-cell-associated antigens (CD20, CD22, and CD79a) and are negative for CD5, CD10, and CD3. Flow cytometry immunophenotyping is a useful ancillary test to prove clonality in these cases.
Papillary thyroid carcinoma is the most common type of thyroid carcinoma, characterized by overlapping nuclei with finely dispersed optically clear chromatin, micronucleoli, eosinophilic intranuclear inclusions and longitudinal nuclear grooves. Some of these nuclear features can be seen in Hashimoto thyroiditis, but the changes are only focal when compared to papillary thyroid carcinomas. Patients with Hashimoto thyroiditis have increased risk for papillary thyroid carcinoma, warranting close clinical follow up.
Supplementary Questions
- Which of the following will be seen in Hürthle cells on ultrastructural examination?
- Lipid droplets
- Mitochondria
- Rough endoplasmic reticulum
- Smooth endoplasmic reticulum
- Tubular cristae
- Which of the following is true in patients with Hashimoto thyroiditis?
- Hashimoto thyroiditis patients have high titers of circulating antibodies to thyroid peroxidase and thyroglobulin.
- Hashimoto thyroiditis patients usually present with hyperthyroidism.
- Most patients are older males.
- Surgical resection is never performed in these patients.
- The majority of the patients have poor prognosis.
- Patients with Hashimoto thyroiditis are at increased risk for which of the following neoplasms?
- Follicular adenoma
- Medullary carcinoma
- Melanoma
- Multiple myeloma
- Papillary thyroid carcinoma
References
- Azizi G, Keller JM, Lewis M, et al. Association of Hashimoto’s thyroiditis with thyroid cancer. Endocr Relat Cancer. 2014;21(6):845-852.
- Hashimoto, H. Zur kenntniss der lymphomatosen verandererung der schilddruse (struma lymphomatosa). Arch Klin Chirugie 1912; 97:219.
- Livolsi VA. Surgical Pathology of the Thyroid. Philadelphia, PA: Saunders:1990.
- Lloyd R, Osamura R, Kloppel G, Rosai J. WHO Classification of Tumours of Endocrine Organs, 4th ed. Lyon, FR: International Agency for Research on Cancer, 2017.
Author
Kirtee Raparia, MD
Surgical Pathology Committee
Kaiser Permanente
Santa Clara, CA
Answer Key
- Mitochondria (b)
- Hashimoto thyroiditis patients have high titers of circulating antibodies to thyroid peroxidase and thyroglobulin. (a)
- Papillary thyroid carcinoma (e)