Clinical Summary
A 45-year-old man presents with a history of abdominal discomfort. Radiologic studies reveal a relatively well-defined 12 cm mass abutting the left adrenal gland. The resected mass shows a smooth tan cut surface with areas of necrosis and hemorrhage. By immunohistochemistry, the lesional cells are positive for CD21 and CD35.
Master List of Diagnoses
- Dedifferentiated liposarcoma
- Follicular dendritic cell sarcoma
- Gastrointestinal stromal tumor
- Inflammatory myofibroblastic tumor
- Metastatic melanoma
- Sarcomatoid carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 22, and is follicular dendritic cell sarcoma in the abdomen.
Criteria for Diagnosis and Comments
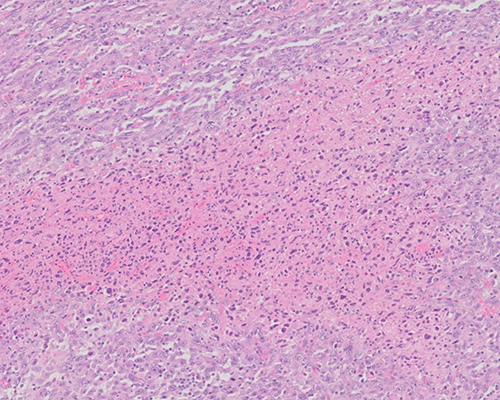
Histologic sections show a diffuse proliferation of oval to spindle-shaped cells with eosinophilic cytoplasm and round to oval nuclei with vesicular chromatin and prominent nucleoli. Mitotic figures and areas of necrosis are present. Lymphocytic infiltrates are present in the background. The histologic features in the context of positive immunostaining for CD21 and CD35 are consistent with follicular dendritic cell sarcoma (FDCS).
FDCS is a rare neoplasm of spindle to ovoid cells with morphologic and phenotypic features of follicular dendritic cells. It typically arises in the lymph nodes (most commonly the cervical, mediastinal or axillary nodes). A third of the cases occur in extranodal sites including the tonsils, nasopharynx, pancreas, liver, and peripancreatic and peritoneal tissues. FDCS occurs at a mean age of 44 years, with equal male-to-female ratio (except the inflammatory pseudotumor-like variant) and presents as a painless, slow-growing mass that is generally asymptomatic except when occurring in the abdomen. The size may range from 1 to 15 cm, largely dependent on the anatomic site, with extranodal tumors reaching a larger size and averaging 7 to 8 cm. On gross examination, FDCS is a well-circumscribed mass with a tan-grey solid surface, with larger tumors showing areas of hemorrhage and necrosis.
Histologically, FDCS is characterized by a diffuse, fascicular, or nodular proliferation of oval to spindle-shaped cells with indistinct borders, eosinophilic cytoplasm, round to oval and elongated nuclei with vesicular chromatin and small nucleoli. A prominent infiltrate of lymphocytes can be spread throughout the tumor cells and in the perivascular spaces. Mitotic activity for low-grade tumors varies from 0 to greater than 10 mitoses per 10 high-power fields (HPF). High-grade histologic features include significant cytologic atypia, high mitotic count (11 to 35 mitoses/10 HPF), and extensive necrosis. High-grade features are associated with deep-seated tumors and recurrent or metastatic behavior.
Immunohistochemical studies are critical to the diagnosis and include positive staining for markers of follicular dendritic differentiation, including CD21, CD35, and CD23. Diffuse staining for clusterin is identified in 100% of cases, including those that are negative for traditional markers of follicular dendritic cell lineage. FDCS shows variable staining for CD68, S100 protein, and EMA, and is typically negative for CD45, CD20, and cytokeratins. FDCS is consistently negative for CD1a, CD3, CD34, CD30, melanocytic markers, desmin, and vascular markers. EBV and HHV-8 are also typically negative in conventional FDCS. FDCS is frequently associated with complex cytogenetic abnormalities, but no consistent or specific aberrations have been established to date. BRAF mutations have been reported in fewer than 20% of the cases.
The inflammatory pseudotumor-like variant of FDCS differs clinically from conventional FDCS by marked female predominance, selective localization in intra-abdominal sites (liver and spleen), presence of systemic symptoms, and indolent behavior. The tumor cells are interspersed with prominent lymphoplasmacytic cells and are consistently EBV positive, raising the possibility that this lesion may be a variant of inflammatory pseudotumor rather than a variant of FDCS.
FDCS occurs in association with Castleman disease in 10% to 20% of patients. Most often, the Castleman disease is of the hyaline vascular type. Castleman disease may precede FDCS, or the two may occur simultaneously. Paraneoplastic pemphigus may also occur in patients with FDCS.
Treatment of FDCS includes surgical excision with or without adjunct radio/chemotherapy. The overall behavior is generally indolent, but 40% to 50% of patients develop recurrence after a prolonged latency period of several years. Distant metastases to lymph nodes, lung and liver occur but are uncommon. Approximately 10% to 20% of patients ultimately die of disease. Worse prognosis is associated with intra-abdominal presentation, high-grade cytologic features, extensive necrosis, and larger size (greater than 6 cm).
A high degree of suspicion is required in the diagnosis of FDCS, since a wide variety of tumor types enter into the differential diagnosis, including carcinoma, melanoma, sarcoma, lymphoma, and other dendritic cell tumors, such as interdigitating dendritic cell tumor. Although FDCS has a distinctive immunophenotype, a broad panel of immunohistochemical stains is often necessary to confirm the diagnosis and exclude other entities.
Interdigitating dendritic cell tumor/sarcoma (IDCT) consistently expresses S100 protein and shows variably weak reactivity for CD68 and CD45. IDCT is negative for CD21, CD23, CD35, CD1a, and langerin.
Dedifferentiated liposarcoma occurs frequently in the retroperitoneum as a large slow-growing mass. Areas of well-differentiated liposarcoma, the presence of lipoblasts, and negative staining for follicular dendritic lineage markers can be helpful to make the distinction from FDCS. In addition, dedifferentiated liposarcoma harbors MDM2 gene amplifications.
Gastrointestinal stromal tumor (GIST) is negative for CD21 and CD35 and positive for CD34 and DOG-1, which are negative in FDCS. In addition, most GIST are also positive for CD117 (c-Kit).
Inflammatory myofibroblastic tumor is composed of myofibroblastic and fibroblastic spindle cells with an inflammatory infiltrate of lymphocytes, plasma cells, eosinophils, and histiocytes. Abundant blood vessels are seen in the background. Ganglion-like myofibroblasts and ALK-1 positivity, when present, are helpful features. The lesional cells are positive for smooth muscle actin, muscle-specific actin, and calponin, but negative for CD21, CD23, and CD35.
Metastatic melanoma is notorious for mimicking many other entities. However, melanoma is positive for melanocytic markers Melan-A and HMB45 and is negative for CD21 and CD35.
Sarcomatoid carcinoma and other carcinomas (primary or metastatic) can be in the differential diagnosis, depending on the site of involvement. However, immunohistochemical stains for follicular dendritic cell lineage are negative in metastatic carcinomas, and most carcinomas, including spindle-cell variants, retain expression of cytokeratins, even if only focally.
Supplementary Questions
- Which of the following is true regarding follicular dendritic cell sarcoma (FDCS)?
- Distant metastases to lymph nodes, lung, and liver are common
- High-grade histologic features are associated with a worse prognosis
- Prognosis is independent of anatomic location
- Surgical resection is of limited value in treatment
- There is no correlation between tumor size and biologic behavior
- Which of the following immunohistochemical profiles is most typical of FDCS?
- CD21(-), CD35(-), smooth muscle actin(+)
- CD21(+), CD35(+), cytokeratin(-)
- CD34(+), DOG-1(+), CD117(+)
- Cytokeratin(+), CD21(-), CD35(-)
- S100(+), Melan-A(+), cytokeratin(-)
- Which of the following is true regarding FDCS?
- BRAF mutation is present in nearly all cases
- Cytogenetic abnormalities alone are sufficient to make the diagnosis
- Histologic features alone are sufficient to make the diagnosis
- Immunoprofile is confirmatory in the appropriate histologic context
- The inflammatory pseudotumor-like variant is marked by male predominance
References
- Chen T, Gopal P. Follicular dendritic cell sarcoma. Arch Pathol Lab Med. 2017,141(4):596-599.
- Cheuk W, Chan J, Shek T, et al. Inflammatory pseudotumor-like follicular dendritic cell tumor. A distinctive low-grade malignant intra-abdominal neoplasm with consistent Epstein-Barr virus association. Am J Surg Pathol. 2001;25(6):721-731.
- Facchetti F, Lorenzi L. Follicular dendritic cells and related sarcoma. Semin Diagn Pathol. 2016;33(5):262-276.
- Grogg KL, Lae ME, Kurtin PJ, Macon WR. Clusterin expression distinguishes follicular dendritic cell tumors from other dendritic cell neoplasms: report of a novel follicular dendritic cell marker and clinicopathologic data on 12 additional follicular dendritic cell tumors and 6 additional interdigitating cell tumors. Am J Surg Pathol. 2004;28(8):988-998.
- Ohtake H, Yamakawa M. Interdigitating dendritic cell sarcoma and follicular dendritic cell sarcoma: histopathological findings for differential diagnosis. J Clin Exp Hematop. 2013;53(3):179-184.
- Shia J, Chen W, Tang LH, et al. Extranodal follicular dendritic cell sarcoma: clinical, pathologic, and histogenetic characteristics of an underrecognized disease entity. Virchows Arch. 2006;449(2):148-158.
- Su Z, Liu G, Liu J, et al. Paraneoplastic pemphigus associated with follicular dendritic cell sarcoma: report of a case and review of literature. Int J Clin Exp Pathol. 2015;8(10):11983-11994.
- Wu A, Pullarkat S. Follicular dendritic cell sarcoma. Arch Pathol Lab Med. 2016;140(2):186-190.
Authors
Vijaya B. Reddy, MD
Surgical Pathology Committee
Rush University Medical Center
Chicago, IL
Answer Key
- High-grade histologic features are associated with a worse prognosis (b)
- CD21(+), CD35(+), cytokeratin(-) (b)
- Immunoprofile is confirmatory in the appropriate histologic context (d)