- Home
- Member Resources
- Pathology Case Challenge
- Adrenal Gland
Clinical Summary
A 45-year-old woman presents to her internist with back pain for the past few months. On further examination a high level of dehydroepiandrosterone sulfate (DHEA-S) in her serum is detected. On computed tomography scan of her abdomen, she is found to have a mass in the left adrenal gland. Gross examination reveals a yellow-tan mass measuring 8 cm in greatest dimension with hemorrhagic and necrotic cut surface. The mass infiltrates into the surrounding adipose tissue. There is a rim of compressed adrenal gland surrounding the mass. Sections from the mass are submitted for microscopic evaluation.
Master List of Diagnoses
- Adrenocortical carcinoma, oncocytic type
- Adrenocortical oncocytoma
- Pheochromocytoma
- Metastatic hepatocellular carcinoma
- Metastatic renal cell carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 18, and is adrenocortical carcinoma, oncocytic type of the adrenal gland.
Criteria for Diagnosis and Comments
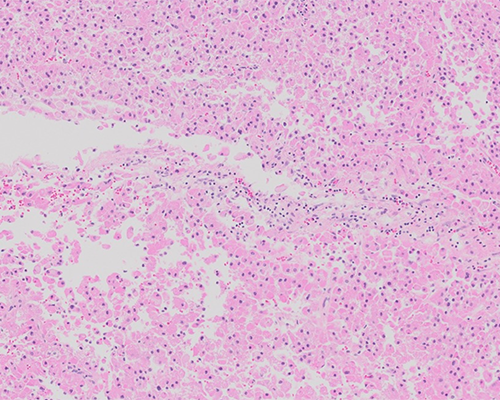
Microscopic sections from the adrenal gland mass show a diffuse proliferation of polygonal cells with abundant granular and eosinophilic cytoplasm, large nuclei, and prominent nucleoli. Some sections show extracapsular extension of the tumor, areas of necrosis, nuclear atypia, and the presence of mitoses. Tumor cells show immunoreactivity with AE1/AE3, are focally positive with inhibin, and are negative for synaptophysin, chromogranin, and S-100 protein. The overall histologic features are suggestive of adrenal cortical carcinoma, oncocytic type.
Various systems have been proposed to distinguish benign from malignant adrenocortical tumors. According to Weiss, adrenocortical carcinoma should have three or more of the following findings: high nuclear grade, eosinophilic cytoplasm (more than 75%), diffuse architecture (more than 33%), necrosis, mitotic figures (more than 5/50 high power field (HPF), atypical mitotic figures, capsular invasion, vascular invasion, and sinusoidal invasion. The use of MIB-1/Ki-67 has also proven helpful in the assessment of benign versus borderline and malignant cases of adrenocortical tumors.
Since most oncocytic tumors already possess three positive criteria (eosinophilic cytoplasm, high nuclear grade, and diffuse architecture), they would all be automatically designated as malignant by the conventional Weiss criteria. Modified Weiss criteria (Lin–Weiss–Bisceglia (LWB) system) recommends the following: an oncocytic tumor is considered malignant if it exhibits one of the following major criteria: a mitotic rate of more than 5 mitoses per 50 HPF, any atypical mitoses, or venous invasion. The tumor is considered to be of uncertain malignant potential (borderline) if it exhibits one of the following minor criteria: large size (greater than 10 cm and/or greater than 200grams), necrosis, capsular invasion, or sinusoidal invasion. Conversely, if none of the above-listed features are present, it is reasonable to call the tumor benign. In summary, for oncocytic adrenocortical neoplasms, the presence of one major criterion indicates malignancy (oncocytic adrenocortical carcinoma), minor criteria only present indicates uncertain potential (borderline), and the absence of all major and minor criteria is indicative of benignancy (adrenocortical oncocytoma).
Surgical excision of these tumors is recommended. Stage plays an important role in the prognosis of these tumors. Overall survival is more than five years for stage I and II tumors.
The differential diagnosis of adrenal cortical carcinoma includes adrenocortical oncocytoma, pheochromocytoma, and metastatic carcinoma such as metastatic hepatocellular and renal cell carcinoma.
The majority of adrenocortical oncocytomas are well-circumscribed tumors with size ranging from 3 to 15 cm. Although they show cytologic atypia, other features of malignancy including necrosis, capsular extension, and vascular invasion are not identified. Ultrastructurally, the conventional adrenal cortical adenoma commonly exhibits abundant smooth endoplasmic reticulum and tubular cristae, while the oncocytic adrenal cortical neoplasm typically shows abundant mitochondria.
Patients with pheochromocytoma may present with throbbing headaches, sweating, palpitations, and chest and abdominal pains which may last from 10 to 60 minutes and may be triggered by positional changes. Pheochromocytomas typically show nests of cells with abundant basophilic cytoplasm, nuclear pleomorphism, presence of nucleoli, and mitoses. Foci of necrosis and areas of increased cellularity can be seen. However, occasionally pheochromocytomas can show oncocytic cells, being confused with adrenal cortical carcinomas, oncocytic type. These tumors are positive for chromogranin and synaptophysin, while the sustentacular cells which surround nests of chief cells are positive for S-100 protein. Electron microscopy would reveal abundant dense-core membrane-bound granules rather than mitochondria.
Renal cell carcinomas and hepatocellular carcinomas can metastasize to adrenal gland. The former scenario needs consideration in patients with Von Hippel–Lindau disease. However, renal cell carcinomas are usually immunoreactive for epithelial membrane antigen, have cytoplasmic vesicles ultrastructurally, and are inhibin negative. Hepar-1 immunostain would exclude the possibility of metastatic hepatocellular carcinoma.
Supplementary Questions
- Which of the following will be seen in tumor cells of oncocytic adrenal cortical carcinomas on ultrastructural examination?
- Lipid droplets
- Mitochondria
- Rough endoplasmic reticulum
- Smooth endoplasmic reticulum
- Tubular cristae
- Which of the following statements is true regarding adrenal cortical carcinomas?
- Adrenal cortical carcinomas are usually associated with inheritable conditions.
- Adrenal cortical carcinomas may show invasion of surrounding vessels, sinusoids, and capsule.
- Ki-67 is not helpful in the assessment of these tumors.
- Surgical resection is not warranted in adrenal cortical carcinomas.
- The majority of the adrenal cortical carcinomas show eosinophilic abundant cytoplasm.
- Which of the following neoplasms is included in the differential diagnosis of oncocytic adrenal cortical neoplasms?
- Melanoma
- Metastatic renal cell carcinoma
- Myelolipoma
- Sarcoma
- Schwannoma
References
- Bisceglia M, Ludovico O, Di Mattiaa, et al. Adrenocortical oncocytic tumors: report of 10 cases and review of the literature. Int J Surg Pathol. 2004;12(3):231-243.
- Hoang MP, Ayala AG, Albores-Saavedra J. Oncocytic adrenocortical carcinoma: a morphologic, immunohistochemical and ultrastructural study of four cases. Mod Pathol. 2002;15(9):973-978.
- Weiss LM, Medeiros LJ, Vickery AL Jr. Pathologic features of prognostic significance in adrenocortical carcinoma. Am J Surg Pathol. 1989;13(3):202-206.
- Lin BT, Bonsib SM, Mierau GW, Weiss LM, Medeiros LJ. Oncocytic adrenocortical neoplasms: A report of seven cases and review of the literature. Am J Surg Pathol. 1998;22(5):603-614.
Author
Kirtee Raparia, MD
Surgical Pathology Committee
Northwestern University
Chicago, IL
Answer Key
- Mitochondria (b)
- Adrenal cortical carcinomas may show invasion of surrounding vessels, sinusoids, and capsule. (b)
- Metastatic renal cell carcinoma (b)