- Home
- Member Resources
- Pathology Case Challenge
- Arm Mass
Clinical Summary
A 44-year-old man presents with a slowly growing 10 cm firm polypoid mass of the right arm. On gross examination, the mass is tan-red and firm, with focal surface ulceration and sloughing of the skin. Sectioning of the mass reveals relatively homogenous tan white surfaces. By immunohistochemistry, the lesional cells are positive for CD34, and cytogenetic studies reveal a t(17;22) translocation.
Master List of Diagnoses
- Dermatofibroma
- Dermatofibrosarcoma protuberans
- Diffuse neurofibroma
- Solitary fibrous tumor
- Synovial sarcoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 23, and is dermatofibrosarcoma protuberans on the arm.
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
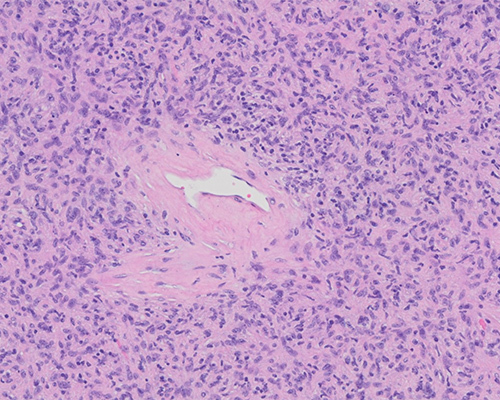
Histologic sections show a diffuse proliferation of uniform spindled cells exhibiting areas of storiform arrangement. There is minimal nuclear pleomorphism and mitotic activity, and no evidence of necrosis. By immunohistochemistry (IHC), the spindle cells are diffusely positive for CD34 and negative for factor XIIIa, S100, CD117, cytokeratin AE1/AE3, EMA, SMA, STAT6, and desmin. These findings, in addition to the cytogenetic studies showing a t(17;22) translocation, are most consistent with dermatofibrosarcoma protuberans (DFSP).
DFSP is a distinctive slow-growing dermal and subcutaneous tumor of intermediate malignancy. Patients are typically in early or middle adulthood. Sites of predilection include the trunk, the proximal extremities, and the head and neck region. DFSP initially manifests as a nondescript cutaneous plaque. Over the course of many years, the plaque progressively grows, ultimately giving rise to one or several protuberant nodules.
Grossly, the tumor appears as a well-circumscribed gray-white nodule involving the dermis and subcutis. The overlying skin may be ulcerated. Necrosis is not a common finding, but hemorrhage and cystic degeneration may be seen.
Microscopically, despite its apparent gross circumscription, DFSP diffusely infiltrates the dermis and subcutis. It characteristically spreads between collagen fibers, expands subcutaneous fibrous septa, and wraps around adnexae and fat cells without destroying them, giving the tumor its characteristic honeycomb appearance. The neoplasm is composed of monomorphic spindle cells arranged in a distinctive storiform or cartwheel pattern. There is little nuclear pleomorphism and no significant mitotic activity. Uncommon histologic findings include myxoid changes, which may cause confusion with a myxoid liposarcoma — giant cells similar to those seen in a giant cell fibroblastoma and atypical fibroxanthoma and focal areas with fibrosarcomatous changes.
DFSP most consistently stains positively with CD34 and is negative for factor XIIIa and S100 protein. Cytogenetically, more than 90% of DFSPs show a t(17;22) translocation leading to formation of a ring chromosome in some tumors. The translocation involves COL1A1 on chromosome 17 and platelet derived growth factor beta (PDGFB) on chromosome 22.
DFSP is a locally aggressive tumor with a high propensity for recurrence (50%). Wide local excision with a 2 cm margin is the standard recommendation, although Mohs micrographic surgery is also a consideration. The presence of fibrosarcomatous areas indicates a more aggressive behavior and increased risk of metastasis. High rates of clinical response have been achieved through the use of imatinib mesylate to inhibit platelet derived growth factor receptors in patients with locally advanced or metastatic DFSP.
Differentiation of DFSP from dermatofibroma (DF), especially the cellular variant, can be quite challenging at times, particularly in small biopsies. In general, DF contains foamy histiocytes, giant cells, and inflammatory cells; demonstrates peripheral entrapment of collagen and overlying epidermal hyperplasia; and does not extend into the subcutis. Most DF are negative for CD34 and positive for factor XIIIa. Other markers have been shown to differentially stain DFSP and other fibrohistiocytic tumors, but their utility in clinical practice has yet to be established. The characteristic cytogenetic abnormality of DFSP is lacking in DF.
Diffuse neurofibroma typically involves the dermis and infiltrates into the subcutis and, therefore, can be a serious consideration in the differential diagnosis of DFSP; however, unlike DFSP, neurofibroma shows diffuse positivity for S100 protein.
Solitary fibrous tumor is a rare mesenchymal tumor that typically involves pleura and is only rarely seen in skin and soft tissues. Although the tumor expresses CD34, solitary fibrous tumor is characterized by a prominent vascular component of ectatic vessels and slit like staghorn vessels exhibiting a hemangiopericytoma-like pattern. A characteristic NAB2::STAT6 fusion is present due to an intrachromosomal inversion at 12q13, which acts as an activator of EGFR1. This is highlighted by the STAT6 immunostain, which is highly sensitive and specific for this tumor.
Synovial sarcoma occurs in the deep connective tissues of the limbs and is characterized by a biphasic pattern that includes an epithelioid cell component in addition to uniform spindle cells. A staghorn-like vascular pattern is typical. Most tumors express EMA and low- and high-molecular cytokeratins. The chromosomal translocation t(X;18) with the SYT::SSX fusion product is quite characteristic of synovial sarcoma.
Supplementary Questions
- Which of the following statements is true regarding dermatofibrosarcoma protuberans (DFSP)?
- It frequently metastasizes to distant organs.
- It is a high-grade malignant tumor.
- It is a slow-growing tumor with a high rate of local recurrence.
- It is typically confined to the dermis without extension into the fat.
- The presence of fibrosarcomatous areas has no prognostic significance.
- Which of the following histologic features is most helpful in distinguishing DFSP from dermatofibroma?
- Biphasic histologic pattern
- Epidermal atrophy
- Infiltration into the subcutis in honey-comb pattern
- Presence of nuclear atypia and necrosis
- Staghorn-like vascular pattern
- Which of the following cytogenetic abnormalities is seen the most frequently in DFSP?
- t(1;2)
- t(1;10)
- t(12;11)
- t(17;22)
- t(X:18)
References
- Bogucki B, Neuhaus I, Hurst EA. Dermatofibrosarcoma protuberans: a review of the literature. Dermatol Surg. 2012;38(4):537-551.
- Elder DE, ed. Lever’s Histopathology of the Skin. 11th ed. Wolters Kluwer, Lippincott Williams and Wilkins;2015;1210-1212,1230-1233.
- Llombart B, Sanmartín O, López-Guerrero JA, et al. Dermatofibrosarcoma protuberans: clinical, pathological, and genetic (COL1A1-PDGFB) study with therapeutic implications. Histopathology. 2009;54(7):860-872.
- Llombart B, Serra-Guillén C, Monteagudo C, López-Guerrero JA, Sanmartín O. Dermatofibrosarcoma protuberans: a comprehensive review and update on diagnosis and management. Semin Diagn Pathol. 2013;30(1):13-28.
- Thway K, Noujaim J, Jones RL, Fisher C. Dermatofibrosarcoma protuberans: pathology, genetics, and potential therapeutic strategies. Ann Diagn Pathol. 2016;25:64-71.
Answer Key
- It is a slow-growing tumor with a high rate of local recurrence. (c)
- Infiltration into the subcutis in honey-comb pattern (c).
- t(17;22) (d)