Clinical Summary
A 55-year-old woman with a history of lung carcinoma presents with a 13 cm breast mass. Grossly, the mass has a spongy hemorrhagic appearance with ill-defined borders. Histologically the tumor is composed of epithelioid cells admixed with hemorrhage. The tumor cells are positive for pan-cytokeratin, EMA, CD31, and ERG.
Master List of Diagnoses
- Atypical vascular lesion
- Capillary hemangioma
- Epithelioid angiosarcoma
- Invasive breast carcinoma of no special type (ductal; not otherwise specified)
- Metastatic lung adenocarcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 11, and is epithelioid angiosarcoma in the breast.
Criteria for Diagnosis and Comments
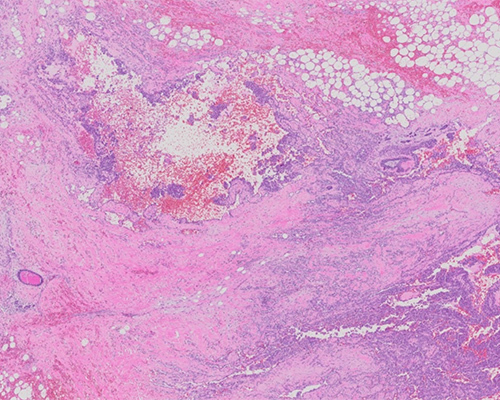
H&E staining shows areas of irregularly anastomosing vessels, with a pseudopapillary and tufting formation with hobnailing of cells in a background of hemorrhage. The cells are large, mildly to moderately pleomorphic, round to polygonal, and epithelioid, with abundant eosinophilic cytoplasm and centrally to eccentrically located nuclei containing prominent nucleoli. Within the nucleus, the chromatin is peripherally marginated, yielding a vesicular appearance. The background shows hemorrhage. The combined histologic features and immunohistochemical (IHC) results are consistent with epithelioid angiosarcoma (AS).
Mammary epithelioid AS can arise from the breast parenchyma either idiopathically (primary/de novo) or following surgery and postoperative radiation for breast cancer (secondary). It can also arise from the overlying skin or the chest wall. Primary mammary AS is rare, with an incidence of approximately 0.05% of all primary malignancies of the breast. However, it is the second most common malignant mesenchymal tumor in the breast. Due to the more frequent use of management options with breast-conserving surgery followed by radiation therapy for carcinoma, secondary AS of the breast has been increasing in incidence.
Clinically, the overwhelming majority of patients with primary AS of breast parenchyma are female and aged between 15 to 75 years (median, 40 years). These painless tumors are usually located deep within the breast parenchyma; however, diffuse breast enlargement can be seen in approximately 12% of patients. A bluish-red discoloration may be identified when the tumor involves the overlying skin. Imaging is usually nondistinctive. Occasionally, primary AS presents with bilateral lesions, but this is thought to represent locoregional metastasis. Secondary AS of the breast associated with radiation therapy is seen in two settings. The first setting is AS occurring in the chest wall subsequent to radiotherapy following mastectomy for invasive breast carcinoma, with a latent interval of 30 to 156 months (mean: 84 to 120 months). These patients are usually older than those with de novo AS (range: 60 to 80 years). In contrast to primary AS, histologically, these cases predominantly involve the skin.
The other setting is development of AS in the breast after lumpectomy and radiotherapy for breast carcinoma. In this scenario, the median latent interval after radiation is 60 to 72 months, but it can occur within 24 months in some cases. Although this type of secondary AS also usually involves the skin, occasionally it can occur in mammary parenchyma or involve both. Many of these lesions are multifocal and may be associated with preceding or synchronous atypical post-radiation vascular proliferations in the breast skin. Patients with secondary AS may have a history or simultaneous presentation of atypical post-radiation vascular proliferation in the breast skin. AS may have nonspecific imaging findings and may not be identified on mammography or ultrasound; magnetic resonance imaging is reportedly more sensitive for detection.
Grossly, the average size of AS is 5 cm (range:1 to 25 cm). It often has a spongy hemorrhagic appearance, with ill-defined borders. Poorly differentiated tumors may have more solid and fibrous-appearing areas. Morphologically, well-differentiated AS consists of anastomosing vascular channels with variably dilated or angulated lumina that dissect through adipose tissue and lobular stroma. The nuclei of the endothelium lining the neoplastic vessels are prominent and hyperchromatic. However, mitoses and multilayering of endothelial cells are infrequent in well-differentiated AS.
On the other hand, poorly differentiated AS is more easily recognized as malignant, since anastomosing vascular channels are intermingled with solid, cellular areas with spindled or epithelioid morphology, often with blood lakes, necrotic foci, and numerous mitoses. Lesions intermediate between these two groups show endothelial multilayering or papillae, as well as readily identified mitoses, but they lack the solidly cellular areas. In high grade or poorly differentiated AS, the malignant endothelial cells may appear epithelioid, as in the present case. The gross and microscopic features of secondary AS are similar to those of primary/de novo AS; the main differences are a higher frequency of cutaneous involvement and a somewhat higher proportion of epithelioid and poorly differentiated tumors.
There are conflicting literature reports on whether the grade distribution varies between the groups. In poorly differentiated AS, diagnosis may be aided by positive IHC staining for CD31, CD34, nuclear ERG, and nuclear FLI1, and sometimes podoplanin (D2-40). Variable expression of pan-cytokeratin and EMA in epithelioid AS may be a diagnostic pitfall.
Activating mutations in the receptor tyrosine kinase gene KDR have been detected in a subset of mammary AS, both sporadic and radiation-associated types. In addition, radiation-associated AS also shows a high level of MYC amplification. Although histological grading was thought to be prognostically important in the past, recent data with more complete follow-up have shown that, similar to AS at other locations, grade fails to show prognostic value, and morphologically low-grade lesions can often metastasize. The lungs, skin, bone, and liver are the most common sites of metastasis. Though rare, axillary lymph nodes can be involved. Median recurrence-free survival and overall survival are less than three years and less than six years, respectively.
Atypical vascular lesion (AVL) of the breast is the main differential diagnosis for low-grade cutaneous AS (cAS). AVL of the breast appears as a skin-colored vesicle or papule, ranging from 0.1 to 2 cm in diameter, and usually develops three years after radiation or surgery. It may be extremely challenging to distinguish AVL from cAS, especially in small or superficial biopsies, because of the overlapping features between the two. AVLs may form irregular vessels, which may appear thin and dilated in the superficial dermis without involving the subcutis or displaying irregular staghorn architecture. Some helpful histologic features to differentiate AVL from cAS are that cAS usually includes necrosis, atypical mitotic figures, and areas of hemorrhage. AVL does not exhibit these features. Phenotypically, AVL is usually cMYC negative by IHC and shows a low Ki-67 proliferative rate.
Invasive breast carcinoma of no special type (ductal; not otherwise specified) is the most common type of breast cancer (approximately 75%). It usually presents as a hard, immovable mass with irregular borders that may radiologically show calcification. Grossly, it varies in size and is firm-hard in consistency, with poor circumscription, stroma with chalky-white streaks, and calcification. In larger tumors, central hemorrhage, necrosis and cystic degeneration may be seen. Infiltration into the overlying chest wall and skin may cause skin dimpling or nipple retraction. Histologically, approximately 80% of cases are associated with ductal carcinoma in situ (DCIS).
Microscopically, tubular and glandular formation by tumor cells is variable based on histologic grade of the tumor. The tumor cells are embedded in desmoplastic stroma admixed with calcification, elastosis, and variable areas of necrosis. The lesions show a high mitotic rate and loss of myoepithelial cell lining, in contrast to benign breast lesions and DCIS. Approximately 30% of ductal carcinoma of the breast shows perineural and/or lymphovascular invasion.
Phenotypically, tumor cells are positive for GCDFP15, pan-cytokeratin, CK8/18, CK7, and EMA. Myoepithelial markers such as p63 and calponin, as well as smooth muscle myosin heavy chain, are negative in invasive tumor cells. The breast biomarkers estrogen receptor (ER), progesterone receptor (PgR), and Her2 are positive in approximately 70%, 55%, and 15% to 30% of tumors, respectively. The presence of expression of E-cadherin is useful for differentiation of ductal carcinoma from lobular carcinoma. Lack of expression of endothelial markers in invasive ductal carcinoma cells helps to differentiate from epithelioid AS.
Capillary hemangiomas tend to be cellular and may mimic AS or superficially resemble pyogenic granulomas. The mean gross size of these hemangiomas is 1 cm. Many of these lesions are detected by mammography. Microscopically, capillary hemangiomas are composed of small vascular channels lined by endothelial cells that may have hyperchromatic nuclei. Fibrous bands are variably present, subdividing the lesion. Larger muscular vessels may be found within and at the periphery of the tumor, apparently constituting branches of a feeding vessel or vessels. These are nonneoplastic muscular vessels with features of arteries and/or veins. Often, the muscular component of these vessels seems malformed or incomplete, and the vessels have a sinuous configuration. The resultant configuration suggests that the hemangioma arose from the feeding vessel.
Hemangiomas from a previous biopsy site may show hemorrhage, and changes from a healing surgical wound may mimic angiosarcoma. One of the helpful histologic features is the presence of a lower mitotic rate (usually less than 5%) in hemangioma compared to AS (usually greater than 20%, even in low-grade tumors). In addition, most hemangiomas tend to have well-circumscribed borders grossly and microscopically, whereas AS have invasive margins.
Poorly differentiated adenocarcinoma and AS can be similar in histologic appearance. Some carcinomas have a pseudovascular pattern. Also, patchy expression of cytokeratins and EMA has been reported in up to 40% of AS, possibly leading to a false diagnosis of poorly differentiated carcinoma. The histologic features of epithelioid AS preclude a definite diagnosis on routine microscopic evaluation of H&E-stained slides. Their sheet-like epithelioid appearance, together with positive cytokeratin staining, may lead to a misdiagnosis of metastatic or primary carcinoma.
The presence of irregular vessels at the periphery of the tumor, intracytoplasmic vacuoles, small areas of hemorrhage and erythrocytes in vascular lumens may serve as diagnostic clues for vascular origin in poorly differentiated AS. Lumina may mimic signet ring cells, but mucin staining will be helpful to differentiate between these two. Moreover, EMA is negative in most noncutaneous AS, while other carcinomas express EMA.
In contrast, carcinomas do not stain with endothelial markers, such as factor VIII, CD31, CD34, ERG, and FLI1. IHC for epithelial and endothelial markers may be helpful for definite diagnosis. For this specific case, although there is overlapping expression of cytokeratin and EMA, the lack of expression of TTF1 and Napsin-A and the presence of endothelial marker expression helps to differentiate epithelioid AS from metastatic adenocarcinoma of lung primary.
Supplementary Questions
- Which of the following is true regarding epithelioid angiosarcoma (AS) tumor cells?
- They are positive for CD31 but always negative for D2-40.
- They are positive for CD34 but negative for FLI1.
- They can be positive for cytokeratin and/or EMA.
- They can show cytoplasmic staining with FLI1.
- They show cytoplasmic staining with ERG.
- Which is/are the most useful feature(s) to favor hemangioma over angiosarcoma?
- Cytologic atypia of endothelial cells
- Presence of blood lakes and/or hemorrhage
- Presence of infiltrative growth pattern
- Presence of necrosis
- Small size, well circumscribed border, and low mitotic activity
- Which of the following is a pattern characteristic of atypical vascular lesion that will distinguish it from angiosarcoma?
- Negative for cMYC, high Ki-67 proliferative index
- Negative for cMYC, low Ki-67 proliferative index
- Positive for cMYC, high Ki-67 proliferative index
- Positive for cMYC, low Ki-67 proliferative index
- Positive for FLI1 and CD31
References
- Leong AS-Y, Cooper K, Leong FJW-M. Manual of Diagnostic Antibodies for Immunohistochemistry. 2nd ed. London, UK: Greenwich Medical Media Ltd; 2003;215-218.
- Tavassoli F, Eusebi V. Tumors of the Mammary Gland. AFIP Atlas of Tumor Pathology. Vol 10. Series 4, Washington, DC: Armed Forces Institute of Pathology; 2009.
- Shustef E, Kazlouskaya V, Prieto VG, Ivan D, Aung PP. Cutaneous angiosarcoma: a current update. J Clin Pathol. 2017;70(11):917-925.
- WHO Classification of Tumors Editorial Board. Breast Tumors. WHO Classification of Tumours. 5th ed. Lyon, France: IARC press; 2019.
Authors
Viren Patel, MD
Surgical Pathology Fellow
UT MD Anderson Cancer Center
Houston, TX
Phyu P Aung, MD, PhD, FCAP
Surgical Pathology Committee
UT MD Anderson Cancer Center
Houston, TX
Answer Key
- They can be positive for cytokeratin and/or EMA. (c)
- Small size, well circumscribed border, and low mitotic activity (e)
- Negative for cMYC, low Ki-67 proliferative index (b)