Clinical Summary
A 67-year-old woman presents with a vague area of thickening in her left breast. Mammographic imaging is unremarkable, and ultrasound reveals an ill-defined mass which is excised.
Master List of Diagnoses
- Gastric signet ring adenocarcinoma
- Invasive carcinoma of no special type (ductal; not otherwise specified)
- Invasive lobular carcinoma
- Lobular carcinoma in situ involving sclerosing adenosis
- Myofibroblastoma, epithelioid variant
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 21, and is invasive lobular carcinoma of the breast.
Criteria for Diagnosis and Comments
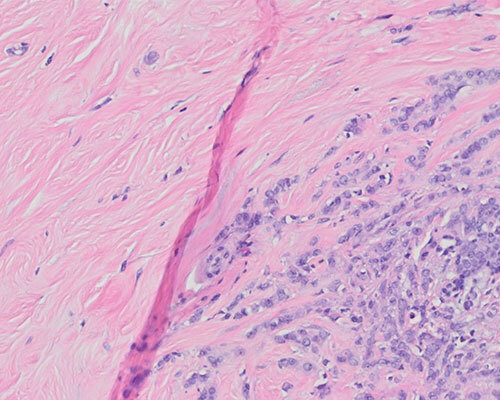
Histologic sections reveal a neoplastic process invading fibrous stroma and adipose tissue as single, non-cohesive cells or cells in a single-file arrangement. The stroma itself lacks a prominent desmoplastic response, and normal architectural features are undisturbed. The invasive cells are small and uniform, with round to oval, often eccentrically placed nuclei. Mitotic figures are rare. These findings are morphologically consistent with a diagnosis of invasive lobular carcinoma (ILC). Rare tubule formation is noted in some sections, and a diagnosis of tubulolobular carcinoma may be considered. Tubulolobular carcinoma is classified as a variant of ILC, according to the 2019 World Health Organization Classification of Tumours of the Breast.
Clinically, ILC often presents as a poorly defined palpable mass or vague area of thickening. Mammography rarely serves to identify ILC, as calcification is not common in this entity. Mammographic findings are subtle, and ultrasound is preferred for both identification and estimation of the size of the lesion. Magnetic resonance imaging (MRI) is considered highly sensitive for detecting ILC, especially when detecting multifocal lesions, which are not uncommon in this entity. However, caution should be used, as it may be prone to false positives and overestimation of lesion size.
The gross presentation of ILC spans a spectrum from rubbery to firm and may be ill-defined or grossly inapparent. In general, ILC consists of small, discohesive cells with uniform cytology. The neoplastic cells may form a concentric pattern around benign ducts and lobules. Mucoid inclusions referred to as intracytoplasmic “lumina” are often identified and are more evident with a mucicarmine stain. Rarely, ILC is accompanied by a lymphocytic reaction.
Classic ILC is most often a low- to intermediate grade lesion. The grade of ILC is based on three histologic characteristics in the Nottingham score: negligible gland formation, monotonous cytology, and rare mitotic activity. Of these three, the mitotic index is the most important prognostic indicator, with a lower mitotic rate associated with better outcomes.
While classic ILC is the most common pattern, the histologic appearance may vary on architectural and cytologic grounds. The solid type maintains a non-cohesive structure while growing in sheets, in addition to increased cellular pleomorphism and mitoses. The alveolar variant consists of aggregates containing 20+ cells separated by fibrovascular stroma. The trabecular variant is similar to classic ILC, but the linear bands are more than two cells thick. Tubulolobular carcinoma is a variant that contains both the classical linear pattern of small, uniform cells, and the formation of small tubules occupying less than 90% of the lesion. The signet ring and pleomorphic variants maintain the growth pattern of classic ILC but differ cytologically. Signet ring morphology is the result of particularly prominent mucinous inclusions in the cytoplasm. Pleomorphic lobular carcinoma may display apocrine or histiocytoid differentiation and, by definition, displays grade 3 nuclear atypia. On occasion, ILC may coexist with invasive carcinoma of no special type (NST), formerly known as invasive ductal carcinoma.
Recent studies of the molecular features of breast lesions have identified recurrent genetic abnormalities and alluded to a common evolution of low-grade lesions that is separate and distinct from high-grade lesions. ILC has been grouped with other low-grade lesions, including flat epithelial atypia, atypical ductal and lobular hyperplasia, lobular carcinoma in situ, ductal carcinoma in situ, invasive mucinous carcinoma, tubular carcinoma, and carcinoma of NST, and has been found to exhibit deletions of chromosome 16q and gains of chromosome 1q. In contrast, high-grade lesions rarely display this specific loss/gain and instead demonstrate more complex karyotypes.
By immunohistochemistry (IHC), the vast majority of ILC are estrogen receptor (ER) positive and many are progesterone receptor (PR) positive. HER2 amplification is extremely rare in ILC, with the exception of the pleomorphic variant. The proliferation rate is generally low when measured by Ki-67. The most characteristic IHC profile concerns a cell-cell adhesion molecule, E-cadherin, located on the gene CDH1 on chromosome 16q. In a majority of ILC, immunoreactivity of E-cadherin is markedly reduced or absent. However, lesions with the classic histologic appearance of ILC should not be reclassified as invasive carcinoma of NST based on E-cadherin expression alone, as aberrant E-cadherin expression is well-reported. p120-catenin, a protein that links E-cadherin to the actin cytoskeleton, fails to localize to the cell membrane as in carcinoma of NST, and instead shows cytoplasmic staining. The use of p120 is extremely helpful to confirm the not-infrequent equivocal E-cadherin staining and, more importantly, provides positive staining in the tumor, which can be crucial in identifying subtle invasion and highlighting tumor extent.
Breast conservation has proven more difficult due to the prevalence of multifocality. Mastectomy is performed more often in patients with ILC, when compared to patients with invasive carcinoma of NST. As expected due to its consistent biomarker phenotype, hormonal therapy was found to be more effective than chemotherapy in the neoadjuvant setting. Breast conservation via lumpectomy should be accompanied by radiation therapy unless the patient has a contraindication. Adjuvant treatment with hormonal therapy should be utilized in the post-surgical period.
Within the first 10 years after diagnosis, ILC patients have similar or better outcomes than those diagnosed with invasive carcinoma of NST. However, long-term outcomes are worse with higher incidences of distant metastases, recurrence, and mortality. Pleomorphic and solid subtypes predict a worse prognosis. Axillary lymph node involvement is less frequent than in invasive carcinomas of NST. ILC metastases have a predilection for bone, gastrointestinal tract, reproductive organs, peritoneum, and meninges, in contrast to invasive carcinoma of NST, which prefers the lungs, liver, and brain.
While the histologic pattern of ILC is often characteristic, a differential diagnosis must still be considered. The monomorphic and discohesive cells combined with the linear pattern of infiltration without prevalent tubule formation should differentiate this lesion from invasive carcinoma of NST. In rare cases where the distinction is unclear, E-cadherin and p120 can be useful.
In the epithelioid variant of myofibroblastoma, tumor cells may be arranged in a linear growth pattern or in alveolar groups and may mimic classical or alveolar ILC. These lesions contain ample fat and rarely may appear invasive at the margins, providing further difficulty in distinguishing from ILC, especially on core needle biopsy. Myofibroblastoma will stain positive for smooth muscle actin, desmin, vimentin, and CD34, but not cytokeratin.
When signet ring morphology is identified in the breast, care should be taken to consider gastric signet ring adenocarcinoma in the differential diagnosis. Primary gastric carcinoma may show a lack of E-cadherin expression. GATA3, mammaglobin, and Gross Cystic Disease Fluid Protein 15 can be helpful, as they are positive in signet ring ILC and typically not expressed in gastric signet ring carcinoma. The gastrointestinal marker CDX2 may also help to distinguish gastric vs. mammary origin.
Sclerosing adenosis involved by lobular carcinoma in situ may present with an infiltrative-like pattern and be mistaken for ILC, especially in a core needle biopsy. However, adenosis will maintain its myoepithelial layer, which can be highlighted by p63 and smooth muscle myosin-heavy chain staining.
Supplementary Questions
- Which of the following immunohistochemical profiles is most commonly found in invasive lobular carcinoma?
- ER(-), PR(-), HER2(+), Ki-67 high, E-cadherin(-), p120 cytoplasmic
- ER(+), PR(+), HER2(-), Ki-67 low, E-cadherin(-), p120 cytoplasmic
- ER(+), PR(+), HER2(-), Ki-67 low, E-cadherin(-), p120 membranous
- ER(+), PR(+), HER2(-), Ki-67 low, E-cadherin(+), p120 cytoplasmic
- ER(+), PR(+), HER2(-), Ki-67 low, E-cadherin(+), p120 membranous
- Which of the following histologic features of invasive lobular carcinoma has been found to correlate most closely with prognosis?
- Intracytoplasmic lumina
- Linear growth pattern
- Mitotic rate
- Nuclear grade
- Tubule formation
- In comparison to invasive lobular carcinoma, invasive carcinoma of no special type (ductal; not otherwise specified) more frequently metastasizes to which of the following sites?
- Bone
- Gastrointestinal tract
- Lung
- Meninges
- Reproductive organs
References
- Abdel-Fatah TM, Powe DG, Hodi Z, Lee AH, Reis-Filho JS, and Ellis IO. High frequency of coexistence of columnar cell lesions, lobular neoplasia, and low grade ductal carcinoma in situ with invasive tubular carcinoma and invasive lobular carcinoma. Am J Surg Pathol. 2007;31(3):417-426.
- Brogi E, Hoda SA, Koerner FC, et al. Rosen's Diagnosis of Breast Pathology by Needle Core Biopsy. 4th ed. Ch 19, p.349-364. Philadelphia, PA: Lippincott Williams & Wilkins. 2017.
- Canas-Marques R, Schnitt SJ. E-cadherin immunohistochemistry in breast pathology: uses and pitfalls. Histopathology. 2016;68(1):57-69.
- Dabbs DJ, Schnitt SJ, Geyer FC, et al: Lobular Neoplasia of the Breast Revisited With Emphasis on the Role of E-Cadherin Immunohistochemistry. Am J Surg Pathol. 2013;37(7):e1-e11.
- Gradishar WJ, Anderson BO, Aft R, et al. NCCN Clinical Practice Guidelines in Oncology, Breast Cancer. National Comprehensive Cancer Network. 2018.
- Hoda SA, Brogi E, Koerner FC, et al. Rosen’s Breast Pathology. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins. 2014;855-892.
- Hortobagyi GN, Connolly JL, D’Orsi CJ, et al. AJCC Cancer Staging Manual. 8th ed (breast edit). Chicago, IL: Springer. 2017.
- WHO Classification of Tumours Editorial Board. Breast Tumours. 5th ed. International Agency for Research on Cancer; 2019.
- Rakha EA. The low nuclear grade breast neoplasia family. Diagnostic Histopathology. 2012;18(3):124-132.
- Schnitt SJ, Collins LC. Biopsy Interpretation of the Breast. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins. 2018;315-326.
Authors
Nena C Wendzel, DO, MS
Surgical Pathology Resident
Walter Reed National Military Medical Center
Bethesda, MD
Justin M Wells, MD, FCAP, LTC MC USA
Surgical Pathology Committee
Walter Reed National Military Medical Center
Bethesda, MD
Answer Key
- ER(+), PR(+), HER2(-), Ki-67 low, E-cadherin(-), p120 cytoplasmic (b)
- Mitotic rate (c)
- Lung (c)