- Home
- Member Resources
- Pathology Case Challenge
- Chest Wall
Clinical Summary
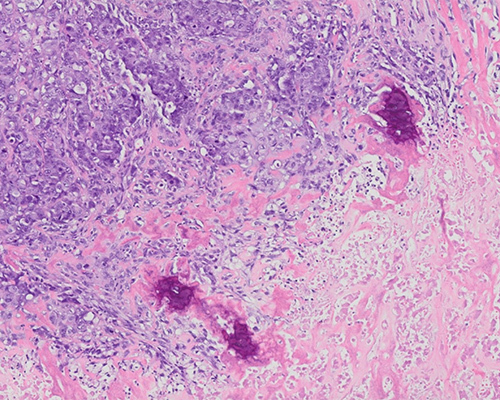
A 52-year-old woman initially diagnosed and treated for breast cancer three years ago presents with a mass in the chest wall. Excision reveals a lobulated, well-circumscribed mass measuring 9 cm. Sectioning reveals a firm, tan tumor with areas of necrosis. The tumor does not involve the overlying skin or the underlying bone. Rare cytokeratin-positive tumor cells are identified on AE1/AE3 cytokeratin staining. The tumor is negative for estrogen receptor (ER), progesterone receptor (PR), and HER2.
Master List of Diagnoses
- Malignant phyllodes tumor
- Metaplastic breast carcinoma with mesenchymal differentiation
- Metastatic carcinosarcoma
- Primary chondroid osteosarcoma
- Radiation-induced osteosarcoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 04, and is metaplastic breast carcinoma with mesenchymal differentiation.
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
Microscopic sections show a high-grade malignant tumor with chondrosarcomatous and osteosarcomatous differentiation, extensive necrosis, and marked nuclear pleomorphism. Clear-cut epithelial differentiation and/or an in situ epithelial component are not identified. Given the focal keratin positivity in conjunction with the patient’s history of a prior breast cancer, this tumor is consistent with a metaplastic breast carcinoma (MBC) with mesenchymal differentiation.
MBC are rare, accounting for 0.2% to 5.0% of invasive breast cancers and primarily affecting women between the ages of 49 to 75. The category encompasses a group of breast cancers that are histologically diverse and can be challenging to diagnose. They are characterized by the presence of an epithelial component with squamous and/or mesenchymal differentiation. There is no consensus on the percentage of the metaplastic component required for the diagnosis of MBC.
The 2019 World Health Organization classification places these tumors into 5 groups based upon the morphology. If more than one pattern is found, as is frequently the case, the tumor is termed a mixed metaplastic carcinoma.
- Low-grade adenosquamous carcinoma: infiltrative well-formed rounded or elongated glandular structures admixed with nests of squamous cells embedded in a spindled stroma. Squamous pearls or squamous cysts may be seen. These tumors are negative for ER, PR, and HER2. Patchy staining for myoepithelial cell markers around the glandular/tubular structures can be seen, with p63 being the most consistently expressed marker. The myoepithelial cells dually express both high and low molecular weight cytokeratins.
- Fibromatosis-like metaplastic carcinoma: bland spindled to plump epithelioid cells arranged in interlacing fascicles in a stroma with varying degrees of collagenization. Focal squamous differentiation can be present. These tumors usually express p63 and high molecular weight cytokeratin, often most pronounced in the epithelioid cells. Low-molecular-weight cytokeratin (CK7) is rarely expressed.
- Squamous cell carcinoma: may be pure squamous cell carcinoma or a mixture of squamous cell and carcinoma of no special type. It typically presents as a cystic cavitary lesion lined by atypical squamous epithelium that invades the surrounding desmoplastic stroma. The differential diagnosis includes a medullary carcinoma with squamous differentiation or a metastatic tumor, usually of skin origin. These tumors may rarely express ER, PR, and HER2.
- Spindle cell carcinoma: moderately to highly pleomorphic spindled cells arranged in a variety of patterns including herringbone, storiform, or short fascicles. The presence of any evidence of epithelial differentiation by either histologic features or immunohistochemistry defines this as a metaplastic spindle cell carcinoma. Identification of either in situ or invasive ductal carcinoma, often noted at the periphery of the tumor, can be an important clue to the diagnosis of metaplastic carcinoma, spindle cell type.
Clinically, MBC often present as a palpable large breast mass with rapid growth. The majority of these tumors are negative for ER, PR, and HER2 and fall into the category of triple-negative carcinomas. Compared to invasive carcinoma of no special type (IC-NST), MBC are less likely to spread to lymph nodes (8% to 40%) and more likely to metastasize to the lung, bones, and brain, suggesting a hematogenous rather than lymphatic pattern of spread. The prognosis of MBC has been difficult to study due to their rarity and the heterogeneity of the tumors within this category. In general, MBC tend to present with larger tumor size and at a higher stage. Pure low-grade adenosquamous carcinoma has been found in some studies to behave in an indolent manner. High-grade adenosquamous carcinoma and its mimic, syringomatous adenoma of the nipple, are locally aggressive tumors. Fibromatosis-like and matrix-producing carcinomas may also have a better prognosis than the others. The mixed metaplastic tumors and spindle cell carcinoma have a worse prognosis. A subset of MBC arise in the setting of neurofibromatosis type 1.
The diagnosis of MBC is relatively straightforward when mesenchymal or squamous differentiation is identified in association with a conventional invasive or in situ mammary carcinoma. In other settings, immunohistochemistry can play an important role in separating MBC from its histologic mimics. As no one marker consistently identifies these tumors, a panel of stains is needed. Most cases of MBC express cytokeratin; however, sometimes a few epithelial markers are needed to prove epithelial differentiation. A useful panel is 34betaE12, CK5/6, CK14, and AE1/AE3. Low-molecular-weight cytokeratins are commonly negative. Cytokeratin expression may be focal. P63 is expressed in greater than 90% of metaplastic breast cancers. CD34, cytokeratin markers, and BCL2 are useful to separate MBCs from malignant phyllodes tumors with sarcomatous overgrowth, as CD34 is negative in MBC. Nuclear beta-catenin can be seen in the fibromatosis-like subtype of MBC, and therefore it cannot be used alone to differentiate it from fibromatosis.
Molecular analysis has demonstrated that most cases of MBC overexpress EGFR. MBCs cluster in the claudin-low spectrum, consistent with the mesenchymal morphology and mutations in the Wnt signaling pathway are common with mutations identified in CTNNB1, APC, or WIXP3. The most common mutation is TP53 (69%), followed by PTEN (11%), ARID1A (11%), and PIK3CA (11%). New targeted therapeutic agents against PIK3CA may make this mutation significant.
Metastatic carcinosarcoma is one of the main entities to be considered in the differential diagnosis. Immunohistochemistry can be helpful. Expression of GATA3 can help support a breast primary, whereas TTF1 might suggest a lung origin. Prior history of a poorly differentiated carcinoma may be the most useful in this setting, as high-grade tumors often lose the immunophenotype commonly expressed in well-differentiated tumors. The prior history of breast cancer in this case was an important factor in helping to make the diagnosis without the use of an extended IHC panel.
Primary mammary osteosarcoma is rare, with some even questioning its existence. It is described in women between the ages of 27 to 89, with a median age of 69. It usually presents as a well-circumscribed tumor. Positive keratin stains would support a carcinoma with sarcomatous differentiation, even if only focally present. The positive keratin stains in this case were very important in making the correct diagnosis.
Malignant phyllodes tumors with sarcomatous overgrowth tumors can show extensive chondroid and osseous differentiation and can be hard to distinguish from MBCs. Immunohistochemical staining for cytokeratin and CD34 can be helpful. Positive keratin stains and negative CD34 support MBC, while a positive CD34 and negative keratin stain support a malignant phyllodes tumor. The positive keratin stain and prior history of breast carcinoma both were important in making the correct diagnosis.
Radiation-induced sarcomas (RIS) can have a variety of morphologies, including osteosarcoma. RIS usually arise two to seven years after irradiation of the breast. Separation from a recurrent metaplastic breast cancer can be problematic. Histologic comparison of the initial breast cancer and the sarcoma can be very helpful. Keratin expression, even if focal, supports a diagnosis of MBC, as in this case.
Supplementary Questions
- Which of the following immunohistochemical panels would be the most helpful in separating a malignant phyllodes tumor from metaplastic breast carcinoma (MBC)?
- AE1/AE3, p63, CD34
- CD34, beta-catenin, AE1/AE3
- CD34, GATA3, smooth muscle actin
- Desmin, smooth muscle actin, p63
- Desmin, STAT6, AE1/AE3
- Which pattern of metastatic spread is more commonly seen in MBC?
- Axillary lymph nodes, brain, liver
- Axillary lymph nodes, contralateral breast, liver
- Axillary lymph nodes, liver, lung
- Bone, brain, liver
- Bone, brain, lung
- Which of the following genes is most commonly mutated in MBC?
- ARID1A
- EGFR
- PIK3CA
- PTEN
- TP53
References
- Cimino-Mathews A, Verma S, Figueroa-Magalhaes MC, et al. A clinicopathologic analysis of 45 patients with metaplastic breast carcinoma. Am J Clin Path 2016;145(3):356-372.
- El Zein DE, Hughes M, Kumar S, et al. Metaplastic carcinoma of the breast is more aggressive than triple-negative breast cancer: a study from a single institution and review of literature. Clin Breast Cancer 2017;17(5):382-391.
- Guerini-Rocco E, Piscuoglio S, Ng CK, et al. Microglandular adenosis associated with triple-negative breast cancer is a neoplastic lesion of triple-negative phenotype harbouring TP53 somatic mutations. J Pathol 2016;238(5);677-688.
- Han M, Salamut A, Zhu L, et al. Metaplastic breast carcinoma: a clinical-pathologic study of 97 cases with subset analysis of response to neoadjuvant chemotherapy. Mod Pathol 2019;32(6)807-816.
- Sotiriou C, Vincent-Salomon A, Rakha EA, et al. Metaplastic Carcinoma. In: WHO Classification Editorial Board, eds. WHO classification of tumours series (5th ed.; vol.2): Breast Tumours. IARC Press; 2019.
- McCart Reed AE, Kalaw E, Nones K, et al. Phenotypic and molecular dissection of metaplastic breast cancer and the prognostic implications. J Pathol 2019;247(2):214-227.
- Rahka EA, Badve S, Eusebi V, et al. Breast lesions of uncertain malignant nature and limited metastatic potential: proposals to improve their recognition and clinical management. Histopathology 2016;68(1):45-56.
- Rahka EA, Coimbra ND, Hodi Z, Juneinah E, Ellis IO, Lee AH. Immunoprofile of metaplastic carcinomas of the breast. Histopathology 2017;70(6):975-985.
- Rakha EA, Tan PH, Shaaban A, et al. Do primary mammary osteosarcoma and chondrosarcoma exist? A review of a large multi-institutional series of malignant matrix-producing breast tumours. Breast 2013;22(1):13-18.
- Tray N, Taff J, Singh B, et al. Metaplastic breast cancers; genomic profiling, mutational burden and tumor-infiltrating lymphocytes. Breast 2018;44;29-32.
Answer Key
- AE1/AE3, p63, CD34 (a)
- Bone, brain, lung (e)
- TP53 (e)