Clinical Summary
A 65-year-old woman presents to the emergency department with watery diarrhea for five days. Her abdomen shows diffuse tenderness on palpation. She is febrile (102˚F) and ill-appearing. She has been bedridden with multiple decubitus ulcers and cellulitis. She was prescribed an antibiotic one month ago to treat the cellulitis. Following admission to the hospital, she continues to decline despite optimal medical management, and a colectomy is performed.
Master List of Diagnoses
- Ischemic colitis
- Necrotizing enteritis
- Pseudomembranous colitis
- Signet-ring cell carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 08, and is pseudomembranous colitis of the colon.
Criteria for Diagnosis and Comments
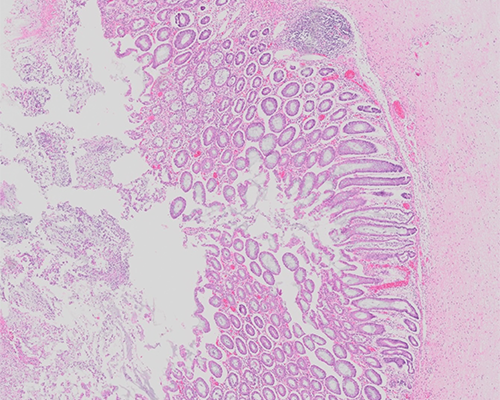
Grossly, the colon shows discrete cream to yellow colored plaques that vary in size from 0.2 to 2.0 cm. The plaques are loosely attached to the erythematous bowel wall. Histologic sections show focal explosive mucosal lesions with mucopurulent exudate. This exudate erupts out of crypts forming mushroom-like clouds with karyorrhectic debris and neutrophils. Superficial crypts show patchy necrosis and are dilated with luminal neutrophils and mucin. The lamina propria is markedly edematous with neutrophilic inflammation. These findings are diagnostic of pseudomembranous colitis (PMC) as a result of Clostridium difficile (CD) infection.
PMC was first described in 1893 as diphtheritic colitis, because of the severe ulceration seen. CD was discovered almost 40 years later. As antibiotic use increased in the mid-twentieth century, the incidence of PMC rose. At the time, it was suspected that the main cause of pseudomembranous colitis was Staphylococcus aureus, one of the most common nosocomial infections. Studies in the 1970s revealed that approximately 20% of patients who were administered clindamycin experienced diarrhea, with half of these patients presenting with pseudomembranous colitis. Later studies showed that CD could secrete powerful toxins, but the effects of said toxins were unknown. CD and its cytotoxin were found in the feces of almost every patient with pseudomembranous colitis but were not present in the feces of healthy subjects. This indicated that the toxins produced by CD caused pseudomembranous colitis. Currently, CD is the second most common anaerobic cause of diarrhea (second to Clostridium perfringens) and the most common cause of nosocomially-acquired diarrhea.
Members of the Clostridium genus are gram negative, anaerobic, spore-forming bacilli encompassing over 100 species. CD is part of the normal flora in the intestine of infants but is rarely present in asymptomatic older children or adults. If the normal intestinal flora is altered by antibiotics, antitumor treatments, or infections, CD colonization can occur. CD produces potent toxins and has been shown to cause acute infectious colitis, antibiotic-associated colitis, pseudomembranous colitis, and neutropenic enterocolitis. Risk factors of PMC are advanced age, prolonged hospitalization, contact with persons with PMC, recent history of surgery (especially gastrointestinal procedures), and malignancy.
Clinical presentation can vary greatly. Some patients present only with diarrhea and show no systemic symptoms, while others show severe systemic toxicity, high fevers, and marked peripheral leukocytosis (up to 50,000/mm3). These symptoms may occur during the course of an antibiotic or may follow weeks later. Thus, there may be a delay in clinical diagnosis if there is a significant lag period.
Multiple antibiotics have been implicated in causing PMC. The most frequently identified antibiotics are cephalosporins, ampicillin, amoxicillin, and clindamycin. Penicillin, macrolides, fluoroquinolones, trimethoprim-sulfamethoxazole, metronidazole, tetracycline, and chloramphenicol have also been shown to be infrequent causes. It has not yet been clearly established whether agents against fungi, mycobacteria, parasites, and viruses can induce CD-associated colitis. The currently associated antibiotics are all orally administered. The antibiotics directly destroy the normal colonic flora, allowing CD to opportunistically colonize the mucosa. Many of the cases of PMC occur in patients over the age of 65 years. A decline in normal flora with aging may increase susceptibility to antibiotics leading to Clostridium colonization. Elderly patients also tend to spend more time in hospitals and may come into contact with the pathogen during their stay.
Two virulence factors are responsible for the majority of CD’s effects. Toxin A and B enzymatically result in cell death by actin cytoskeleton disruption. Tight junctions become permeable causing the significant osmotic diarrhea. Neutrophils and cytokines are directly upregulated by the toxins, further increasing the edema. CD toxin can be assayed serologically to support PMC diagnosis. Additionally, polymerase chain reaction assays can also be used to detect the gene regulating the toxin production.
PMC shows tan well-defined areas on endoscopic exam. Often, the lesions show a significant, sharp demarcation between the abnormal plaques and normal mucosa. The plaques range from the size of a pinpoint to total confluence of the colon. When the lesions are small, multiple biopsies from endoscopically normal and abnormal areas are often needed for diagnosis. The ileum tends to be spared, well-delineated from the affected colon at the ileocecal valve. As the lesions resolve, they often form small, discrete ulcerated areas.
Histologically, small surface erosions of the superficial crypts with overlying accumulation of neutrophils, fibrin, mucus, and necrotic epithelial cells (summit lesion) are seen. The inflammatory exudate erupts from the degenerating crypts in an explosive or mushroom-like configuration. Endothelial damage results in small areas of necrosis in the surface epithelium. The eruption of neutrophils, nuclear debris, and other inflammatory elements from the lamina propria onto the epithelium leads to the characteristic pseudomembrane formation.
Pseudomembranes can be small and scattered among areas of normal or erythematous mucosa. Pseudomembranes may also confluence to cover the entirety of the mucosa. The crypt bases most commonly remain intact. Particularly in severe cases, goblet cells may slough and resemble signet cell carcinoma. Small biopsy specimens may lack the pseudomembrane but retain neutrophilic inflammation in superficial glands (with intact crypts) and show lamina propria edema. Long standing or severe cases may show complete loss of the mucosa with transmural involvement. Biopsies of patchy PMC may show nonspecific active colitis with or without crypt abscesses and may require additional biopsy material, laboratory testing (serology, toxin assays, etc), or clinical history to confirm diagnosis.
Oral vancomycin or metronidazole is typically the drug of choice in treating PMC. When the offending agent causing PMC can be identified, it should be discontinued. If patients are unable to tolerate standard antibiotic therapy, fecal transplants have proven effective in recolonizing the gut with normal flora, which in turn can outcompete CD.
PMC most often resembles ischemic colitis (IC). Pseudomembranes may be present in both entities. The pseudomembranes seen in IC are more commonly small and focal, often forming a mass-like lesion. Thus, an endoscopy showing large pseudomembranes favors the diagnosis of PMC. Atrophic or withered-appearing microcrypts with underlying lamina propria hemorrhage are suggestive of IC. Hyalinization of the lamina propria is a strong indicator of ischemia. Transmural necrosis is often absent in PMC, occurring more frequently in IC. Serology for CD can assist in ruling in PMC, but may lead to false negative results in early or mild cases. A thorough history, including recent medication changes or evidence of additional peripheral vascular disease, can be helpful in reaching a prompt and accurate diagnosis.
Clostridium perfringens associated necrotizing enteritis (NE) also must be considered in cases of PMC. Dusky, ulcerated mucosa is typically seen on endoscopy. Histologically, there is significant necrosis of the mucosa with edema. The crypts become atrophic with an associated neutrophilic infiltrate. Perforation can occur when the inflammation becomes transmural. The diagnosis is made based on additional laboratory and clinical findings specific to C. perfringens.
In cases where a significant number of goblets cells have been sloughed, signet cell carcinoma (SCC) must be considered. Signet cell changes may be seen in a variety of inflammatory conditions including PMC. Cytologic features are not helpful, as nuclear atypia is not generally seen in SCC. The signet cells in SCC show lamina propria infiltration. Reactive signet cell changes are primarily present in crypts and can be seen along the epithelial surface of glands. E-cadherin expression is lost in SCC and retained in reactive signet cells. p53 expression is also seen in SCC and is not present in signet cell change. Ki-67 may display some utility in SCC, typically showing a higher proliferation index as compared to reactive changes.
Supplementary Questions
- Which of these histologic findings favor the diagnosis of pseudomembranous colitis in a biopsy specimen?
- Atrophic crypt lumina
- Hyalinization of the lamina propria
- Marked nuclear atypia
- Relatively well-preserved crypt bases
- Transmural necrosis
- Which of these statements regarding the natural history of pseudomembranous colitis is correct?
- Always occurs within 72 hours of beginning an antibiotic
- Most commonly associated with parenteral piperacillin/tazobactam
- Most often caused by gram-negative rods
- Often treated by oral vancomycin or metronidazole
- Typically observed in patients younger than 10 years old
- Which of the following statements is true regarding signet cell carcinoma?
- The signet cells are positive for CD68.
- The signet cells are usually confined to the glandular epithelial surface and crypts.
- The signet cells show prominent lamina propria infiltration.
- The signet cells show staining for E-cadherin and are negative for p53.
- The signet cells show very low mitotic index (decreased Ki-67 staining).
References
- Borriello SP. Clostridial disease of the gut. Clin Infect Dis. 1995;20 Suppl 2:S242-S250.
- Cerilli LA, Greenson JK. The differential diagnosis of colitis in endoscopic biopsy specimens: a review article. Arch Pathol Lab Med. 2012;136(8):854-864.
- Chyung JW, Shin DG. Localized pseudomembranous colitis in the cecum and ascending colon mimicking acute appendicitis. World J Gastrointest Surg. 2013;5(5):156-160.
- Dignan CR, Greenson JK. Can ischemic colitis be differentiated from C difficile colitis in biopsy specimens? Am J Surg Pathol. 1997;21(6):706-710.
- Farooq PD, Urrunaga NH, Tang DM, Von rosenvinge EC. Pseudomembranous colitis. Dis Mon. 2015;61(5):181-206.
- Jain D. Enteric infections and associated diseases. In: Riddell R, Jain D, eds. Lewin, Weinstein and Riddell's Gastrointestinal Pathology and Its Clinical Implications. Lippincott Williams & Wilkins. 2014; Chapter 19.
- Kendrick JB, Risbano M, Groshong SD, Frankel SK. A rare presentation of ischemic pseudomembranous colitis due to Escherichia coli O157:H7. Clin Infect Dis. 2007;45(2):217-219.
- Lamps L. Bacterial Gastrointestinal Infections. In: Procop GW, Pritt B, eds. Pathology of Infectious Diseases. Saunders. 2014; Chapter 16.
- Surawicz CM, Mcfarland LV. Pseudomembranous colitis: causes and cures. Digestion.1999;60(2):91-100.
- Wang K, Weinrach D, Lal A, et al. Signet-ring cell change versus signet-ring cell carcinoma: a comparative analysis. Am J Surg Pathol. 2003;27(11):1429-1433.
Authors
Archi Patel, MD
Pathology Resident
East Tennessee State University
Johnson City, TN
J. Clint Stanfill, MD
Surgical Pathology Committee
East Tennessee State University
Johnson City, TN
Answer Key
- Relatively well-preserved crypt bases (d)
- Often treated by oral vancomycin or metronidazole (d)
- The signet cells show prominent lamina propria infiltration. (c)