Clinical Summary
A 65-year-old woman presents to the emergency department with fever, abdominal cramping, and non-bloody diarrhea. The patient reports a recent sinus infection with antibiotic use. She acutely decompensates and is found to have leukocytosis and septic shock. A hemicolectomy is performed.
Master List of Diagnoses
- Clostridioides difficile colitis
- Collagenous colitis
- Ischemic colitis
- Signet ring cell carcinoma
- Ulcerative colitis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 17, and is Clostridioides difficile colitis in the colon.
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
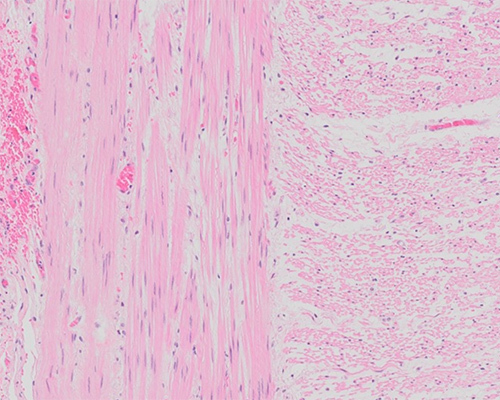
The diagnosis is Clostridioides (formerly Clostridium) difficile colitis. This diagnosis falls into the differential diagnoses of the pseudomembranous colitis inflammatory pattern, which is seen on the provided slide. The colonic mucosa is distorted by ballooned crypts that are filled with neutrophils, sloughed epithelium, and necrosis. At the surface, these contents spill and ultimately come together with fibrin and mucin to compose the hallmark laminated pseudomembranes that overlie the epithelium. This appearance has been termed “volcano lesion.” Necrosis between the crypts can be seen, which can progress to full-thickness mucosal necrosis in more severe cases.
Pseudomembranous colitis is most commonly induced by C. difficile infection. The patients are typically older, but infection can occur at younger ages. Idiopathic inflammatory bowel disease patients have a higher incidence of infection. Additionally, surgical patients, prolonged hospital stay, or long-term facility patients and immunodeficient patients are all at increased risk of infection. Proton pump inhibitor use has also been shown to increase the risk of infection. As the normal colonic flora prevents infection, a disturbance such as recent antibiotic use is commonly identified. Chemotherapeutic or immunosuppressive agents can have the same effect. Classically, C. difficile colitis-associated antibiotics are clindamycin and fluroquinolones, but many different classes of antibiotics have been implicated.
The organism is an obligate anaerobe Gram-positive rod that can form spores. The spore forms are an important mechanism for transmission. A common sequence of events has been found to drive a clinically relevant infection: antibiotic use disrupts the colonic flora and colonization by C. difficile follows, which then leads to toxin production. Colonization by C. difficile is not enough to induce symptoms, as it is not an invasive organism. There is evidence that asymptomatic colonization may actually confer immunologic protection and that the waning effects of the protection in later decades could be part of the reason for the disease predominance in the elderly. As the presence of the bacteria alone is not sufficient for disease, stool culture for C. difficile is therefore not an effective testing method for C. difficile infection. Toxin A and Toxin B are the exotoxins produced by most disease-causing strains.
The diagnosis of Clostridioides difficile infection is dependent on both (1) the presence of diarrhea or radiologic evidence of ileus or toxic megacolon and (2) positive stool test for toxigenic C. difficile or its toxins, or colonoscopy/histologic evidence of pseudomembranous colitis. C. difficile infection can cause a widely variable disease presentation. The spectrum ranges from mild diarrhea to toxic megacolon, with some patients not having any diarrhea at all. Testing for C. difficile infection includes testing for the bacteria or the toxins. The gold standard is toxigenic culture for toxigenic C. difficile or cell cytotoxicity assay for detecting Toxins A or B. However, both of these are resource-intensive and can take more than 24 - 48 hours for a result. Enzyme immunoassay (EIA) for detecting glutamate dehydrogenase, produced by both nontoxigenic and toxigenic strains, with confirmatory EIA for Toxins A or B is a rapid method with turnaround time under an hour. Nucleic acid amplification testing to detect toxin genes (tcdB or tcdC) can be performed in 1 - 3 hours.
The severity of the infection dictates treatment. For most mild to moderate infections, a course of metronidazole or vancomycin is indicated. If the patient is still on a course of the original offending antibiotic, it should be stopped whenever possible. Fidaxomicin is a relatively new antibiotic that has been shown to be noninferior to vancomycin. Fecal microbiota transfer, involving seeding of the gastrointestinal tract with a donor’s stool, has been shown to have high response rates for treating C. difficile infection in conjunction with vancomycin compared to vancomycin usage alone. Potential immunotherapy is evolving, with use of monoclonal antibodies against C. difficile toxins A and B as well as anti-C. difficile toxoid vaccine. However, as the severity increases, the indication for surgical intervention does as well. Operating before the patient develops organ dysfunction/failure or before vasopressors are needed for management of shock generally results in the best outcomes. Mortality for total colectomy with severe, complicated C. difficile infection may approach 30% - 50%. It is necessary in cases of toxic megacolon, perforation, or peritonitis. Before then, it can be difficult to determine which patients will be unsuccessful with medical management alone. Subtotal colectomy remains the definitive surgical treatment.
The gross examination findings of pseudomembranous colitis can be found at any segment of bowel to include the small bowel and appendix. The rectum may be spared. The entire colon can be involved, whether diffusely, segmentally, or patchily, and is covered with yellow-white pseudomembranes. When the membranes are disrupted, bleeding occurs. In the absence of grossly apparent pseudomembranes, the typical histologic patterns may still be seen.
As previously mentioned, pseudomembranous colitis is a histologic inflammatory pattern with a differential diagnosis. The most common setting is C. difficile infection. However, there are a variety of less common causes that should be considered in the setting of C. difficile-negative or refractory pseudomembranous colitis. Chemicals and medications, infections, inflammatory conditions and vascular conditions have all been implicated. Examples of chemicals and medications include cocaine with vasoconstrictive effects and chemotherapeutic agents that can be toxic to the bowel. Ischemic colitis, a diagnostic option for this case, can also present with pseudomembranes but is typically seen in the elderly or debilitated with risk factors such as cardiovascular disease and would not have the positive C. difficile toxin testing. Other types of infection can cause pseudomembranes, notably E. coli O157:H7 and cytomegalovirus. Collagenous colitis and inflammatory bowel disease, other diagnostic options for this case, have both been associated with pseudomembranes, but their more classic histologic patterns are usually present as well, making them unlikely choices for this case. Behçet disease has also been associated with the formation of pseudomembranous colitis.
The last diagnostic option for this case was signet ring cell carcinoma, given the appearance of the degenerating goblet cells; however, these cells retain their position within the normal mucosal architecture with no evidence of an invasive process.
In summary, pseudomembranous colitis can be seen in a variety of settings. The pattern is not synonymous with C. difficile colitis, although C. difficile is the most often underlying cause. C. difficile colitis can have a range of clinical presentations from asymptomatic to toxic megacolon. It requires disruption to the normal colonic flora to colonize, an important aspect in proper antibiotic stewardship.
Supplementary Questions
- Which of the following is true regarding Clostridioides difficile infection?
- C. difficile is the second most common cause of pseudomembranous colitis.
- Clindamycin and fluoroquinolones are the only antibiotics linked to C. difficile infection.
- Pathogenesis of C. difficile is dependent on toxin production, including Toxins A and B.
- Stool culture is adequate for diagnosing C. difficile infection.
- Toxin G is the most pathogenic toxin of C. difficile.
- Which of the following etiologies has been associated with pseudomembranous colitis?
- Cocaine usage
- Irritable bowel syndrome
- Mycobacterium tuberculosis infection
- Rheumatoid arthritis
- Small cell carcinoma
- Which of the following is true regarding therapy for C. difficile infection?
- Fecal microbiota transplant alone is curative for severe, complicated C. difficile infection.
- For most patients with mild to moderate C. difficile infection, metronidazole and vancomycin are considered first-line medical therapies.
- If a patient is on antibiotic therapy when C. difficile infection is confirmed, the treatment must be continued until the end of the regimen.
- Mortality for total colectomy in patients with severe, complicated C. difficile infection is low (around 5%).
- Surgical intervention should be saved until the patient manifests organ dysfunction or failure.
References
- Cerilli LA, Greenson JK. The differential diagnosis of colitis in endoscopic biopsy specimens: a review article. Arch Pathol Lab Med. 2012;136(8):854-864.
- Farooq PD, Urrunaga NH, Tang DM, von Rosenvinge EC. Pseudomembranous colitis. Dis Mon. 2015;61(5):181-206.
- Jessurun J. The Differential Diagnosis of Acute Colitis: Clues to a Specific Diagnosis. Surg Pathol Clin. 2017;10(4):863-885.
- Kodadek LM, Lipsett PA. Prevention and Treatment of Clostridioides difficile Enterocolitis. Adv Surg. 2018;52(1):29-42.
- Lamps LW. in Iacobuzio-Donahue C and Montgomery E, eds., Gastrointestinal and Liver Pathology, a volume in the series Foundations in Diagnostic Pathology, 2nd Edition Elsevier Saunders. 2012: Chapter 9, 320-322.
- Lamps LW. in Odze RD and Goldblum JR, eds., Odze and Goldblum Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas, 3rd Edition. Elsevier Saunders. 2015: Chapter 4, 67-70.
- Tang DM, Urrunaga NH, Von Rosenvinge EC. Pseudomembranous colitis: Not always Clostridioides difficile. Cleve Clin J Med. 2016;83(5):361-366.
Answer Key
- Pathogenesis of C. difficile is dependent on toxin production, including Toxins A and B. (c)
- Cocaine usage (a)
- For most patients with mild to moderate C. difficile infection, metronidazole and vancomycin are considered first-line medical therapies. (b)