Clinical Summary
A 65-year-old right-handed woman with a long-standing history of headaches presents to the emergency room after having a witnessed seizure. A computed tomography scan shows a uniform, contrast-enhancing, extra-axial, parasagittal, dural-based mass. A biopsy is performed.
Master List of Diagnoses
- Clear cell renal cell carcinoma metastases
- Diffuse astrocytoma
- Hemangioblastoma
- WHO grade I meningioma
- WHO grade II meningioma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 39, and is a cranial WHO grade I meningioma.
Criteria for Diagnosis and Comments
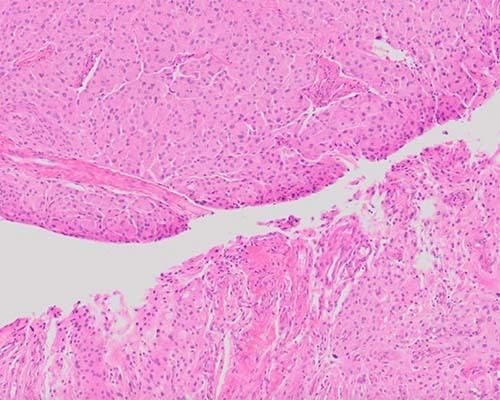
The diagnosis is a WHO grade I meningioma. This tumor has epithelioid, medium-sized lobules, partially demarcated by thin collagenous septa. Additionally, in variably sized foci depending on the slide, there are cobweb-like spaces with elongated processes surrounding them. This tumor did not have increased mitotic activity, and the pattern most consistent with its architectural features would be meningothelial with microcystic features.
WHO grade I meningiomas are benign lesions that are slow growing. They arise from the meningothelial cells of the arachnoid layer. Meningioma is the most common intracranial neoplasm in adults. The median age of patients that have a meningioma is 65 years. Females are at greater risk than males (at a ratio of 1.7-2.1:1); however, males are at greater risk for grade II and grade III lesions.
Most meningiomas arise sporadically, but ionizing radiation is an established risk factor, and they can also arise in the setting of neurofibromatosis type 2. The evidence for increased risk from endogenous/exogenous hormones is weak. Pregnancy can induce rapid growth of a meningioma, but the underlying mechanism is more commonly due to hemodynamic changes rather than a hormonally driven tumor cell proliferation. Presenting symptoms are nonspecific and frequently include headaches and seizures. The underlying etiology of these neurological findings is most commonly due to compression of adjacent structures, rather than overt invasion or extension of the tumor into brain parenchyma.
The most common locations for meningiomas are intracranial, intraspinal, or orbital. The more common sites within the skull include the cerebral convexities, olfactory grooves, sphenoid ridges, para/suprasellar regions, optic nerve sheath, petrous ridges, tentorium, and posterior fossa. The tumors are often found parasagittally, lying along the falx and venous sinuses. The thoracic region is the most common location for spinal meningiomas. The atypical and anaplastic meningiomas most commonly affect the convexities and are not typically found on the skull base.
On MRI, meningiomas are isodense and uniformly contrast-enhancing dural masses. Cyst formation and peritumoral cerebral edema can occur. Neuroimaging is not entirely specific for diagnosing meningiomas or predicting their behavior. Metastases are uncommon, occurring in about 1:1000 meningiomas, and are most often seen in the setting of a grade III meningioma. The lung, pleura, bone, or liver are common locations for metastases.
Grossly, these tumors tend to be rubbery to firm with defined borders. Some may have a lobular appearance, and often have a wide dural attachment. Meningiomas can also grow as an “en plaque meningioma,” where they are broad and flat. This pattern is seen especially in meningiomas growing along the sphenoid wing. Other gross features include a sand-like or gritty texture that indicates the presence of psammoma bodies. Hyperostosis may be induced by meningioma invasion of the skull. Infiltration of the tumor around cerebral arteries and into the skin or extracranial compartments, including the orbit, can also be seen.
Meningiomas are graded as WHO I-III based on histologic subtype, specific histologic criteria, or both. Atypical meningiomas have equal to or greater than 4 and less than 20 mitotic figures per 10 high power fields (HPFs). Anaplastic meningiomas have greater than 20 mitotic figures per 10 HPFs. The microscopic appearances of meningiomas can be quite varied. There are distinct subtypes, and the majority behave in a benign fashion. Based on histologic appearance, there are six recognized subtypes that are automatically graded as a grade II or III. The following are subtypes included in the 2017 WHO classification:
WHO grade I lesions:
- Meningothelial
- Fibrous/fibroblastic
- Transitional/mixed
- Psammomatous
- Angiomatous
- Microcystic
- Secretory
- Lymphoplasmacyte-rich
- Metaplastic
WHO grade II lesions:
- Chordoid
- Clear cell
- Atypical
WHO grade III lesions:
- Papillary
- Rhabdoid
- Anaplastic
The Master List of Diagnoses for this tumor includes a WHO grade II meningioma. However, this tumor does not have the histologic subtype or mitotic activity that would upgrade it to a grade II lesion. Other tumors could be considered in the differential diagnosis.
Hemangioblastomas classically appear as a proliferation of capillaries in a background of large atypical stromal cells. The vessels vary in size and are closely packed. The stromal cells have pink to clear cytoplasm with fine vacuoles, which contain lipid. The tumor in this case, while having foci of cells with clear cytoplasm, lacks vascular proliferation and has a much more epithelioid appearance. Additionally, hemangioblastomas are more commonly located in the spinal cord and cerebellum.
Diffuse astrocytoma consists of well-differentiated fibrillary astrocytes that exist in a loosely structured tumor matrix. The cells in this case are epithelioid and exist in an organized lobular fashion. Again, the location of diffuse astrocytomas helps to separate them from this tumor. They can be found anywhere in the central nervous system but are most commonly supratentorial within the frontal lobes.
Clear cell renal cell carcinoma is a tumor composed of pockets of clear or eosinophilic cells with vessel formation. Although lungs and liver are the most common sites for metastases, metastases to the brain do occur. However, the metastases are not usually dural based, as is this tumor. Additionally, a meningioma lacks the vessel architecture of renal cell carcinoma and, in this case, is not predominated by a clear cell population.
When doubt about the diagnosis exists, immunohistochemical staining may be performed. Meningiomas are positive for vimentin, epithelial membrane antigen (EMA), and somatostatin receptor 2A. Progesterone receptor (PR) can be identified in all types of meningioma but is less prominent in grade II and III meningiomas; therefore, PR status can be viewed as a risk-predictive marker. A similar pattern is found with EMA: the higher the grade, the lower the reactivity with EMA.
Supplementary Questions
- Which of the following is classified as a WHO grade II meningioma?
- Anaplastic meningioma
- Atypical meningioma
- Metaplastic meningioma
- Microcystic meningioma
- Rhabdoid meningioma
- Which of the following hereditary tumor syndromes includes meningioma as a component?
- Li-Fraumeni syndrome
- Muir-Torre syndrome
- Neurofibromatosis type 1
- Neurofibromatosis type 2
- Tuberous sclerosis
- Which of the following tumors most commonly exhibits a combination of positive epithelial membrane antigen and progesterone receptor?
- Diffuse astrocytoma
- Hemangioblastoma
- Grade I meningioma
- Renal cell carcinoma
- Vestibular schwannoma
References
- Brat D, Parisi J, Kleinschmidt-DeMasters B, et al. Surgical neuropathology update: a review of changes introduced by the WHO classification of tumours of the central nervous system, 4th edition. Arch Pathol Lab Med. 2008;132(6):993-1007.
- Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. (Eds): WHO Classification of Tumors of the Central Nervous System (Revised 4th Edition). Lyon, FR:IARC:2016.
- Prayson R, Neuropathology. Philadelphia, PA:Elsevier;2012.
- Shibuya M. Pathology and molecular genetics of meningioma: recent advances. Neurol Med Chi. 2015;55(1):14-27.
Author
Margaux M Canevari, DO, MS, CPT MC USA
Surgical Pathology Resident
Walter Reed National Military Medical Center
Bethesda, MD
Justin M Wells, MD, LTC MC USA
Surgical Pathology Committee
Walter Reed National Military Medical Center
Bethesda, MD
Answer Key
- Atypical meningioma (b)
- Neurofibromatosis type 2 (d)
- Grade I meningioma (c)