Clinical Summary
A 47-year-old hypertensive man without a prior history of cardiac disease presents comatose and in cardiopulmonary arrest. Electrocardiogram shows ventricular fibrillation. A transthoracic echocardiogram (TTE) demonstrates global hypokinesis, a markedly dilated right ventricle, moderate tricuspid regurgitation, and an ejection fraction of 13%. His hospital stay is complicated by acute renal failure and progression to anoxic brain injury and death. An autopsy is performed. Grossly, there is cardiomegaly (heart weight: 1,000 grams) with biventricular dilatation and borderline myocardial hypertrophy. Coronary arteries do not show significant atherosclerosis. Mitral and tricuspid valves are dilated, but there are no vegetations.
Master List of Diagnoses
- Catecholamine induced injury
- Eosinophilic myocarditis
- Giant cell myocarditis
- Lymphocytic myocarditis
- Sarcoidosis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 32, and is lymphocytic myocarditis in the heart.
Criteria for Diagnosis and Comments
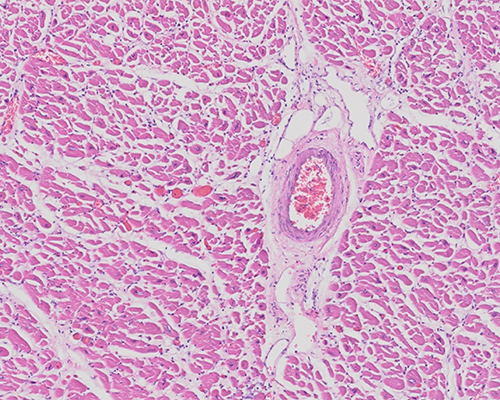
Sections show a multifocal interstitial mononuclear infiltrate, comprised predominantly of lymphocytes admixed with few plasma cells and rare eosinophils. Varying degrees of endocardial and epicardial inflammation is present. Patchy foci of subendocardial coagulative necrosis are present. No well-formed granulomas are seen. Immunohistochemical stains demonstrate the lymphocytes to be predominantly CD3 positive T-cells and only scattered CD20 positive B-cells. Clinical history and morphological and immunohistochemical findings are compatible with the diagnosis of lymphocytic myocarditis.
Myocarditis may present with focal or diffuse involvement of the myocardium resulting in acute, subacute, or chronic disease. Myocarditis is considered a disease of infants, children, and young adults. The prototypical patient with acute viral myocarditis is a young individual presenting with progressive dyspnea, chest pain (suggestive of pericarditis), palpitations, and signs of cardiac failure a few days to weeks after a viral syndrome. A small subset of patients present with fulminant myocarditis and progress to cardiogenic shock as well as multi-organ failure. Myocarditis can result from multiple causes but is most often attributed to infective agents that injure the myocardium through direct or indirect mechanisms. Autoimmune disorders, exogenous agents such as radiation, drugs (doxorubicin, anthracyclines), black widow spider bites, and chemicals are other causes of myocarditis.
Viruses are the most common pathogens for the infectious causes with enteroviruses, including Coxsackie virus, being most frequently implicated in North America and Europe. Other well-established causes include other viral (Parvovirus B-19, human herpesvirus 6, adenovirus, influenza, Epstein-Barr, cytomegalovirus, Human immunodeficiency virus and Hepatitis C), rickettsial (Rocky Mountain spotted fever, Q fever, Lyme disease), bacterial (Mycobacteria spp., Corynebacteria spp.), protozoal (Trypanosoma Cruzi, Toxoplasma spp.), and helminthic (Trichinella spiralis) infections. A causative link to viruses is often difficult to prove as viral cultures and serology have low sensitivity; however, molecular techniques have increased the scope of detection of viruses in cardiac tissues. It is not clear if the viruses discovered through molecular techniques are indeed pathogenic or innocent bystanders. In general, viruses infect the heart via specific transmembrane receptors, such as the coxsackie-adenovirus receptor. Other common but noninfectious causes of myocarditis include autoimmune disorders such as systemic lupus erythematosus (SLE), Wegener’s granulomatosis, and giant cell arteritis.
Lymphocytic myocarditis is a cause of sudden cardiac death (due to atrio-ventricular block and ventricular arrhythmia) in 15% to 20% of children and young adolescents. Grossly, a range of findings from normal appearing heart to four-chamber dilatation with ventricular pallor and softening may be seen, depending on the etiology and duration of the illness. Fibrinous pericarditis may be noted and does not necessarily implicate a bacterial pathogenesis. Fibrosis typically shows a random or subepicardial distribution. Pericardial effusion may be present.
In autopsy cases/explanted hearts, microscopy shows diffuse inflammation of the myocardium with necrosis and/or degeneration of the cardiac myocytes. The inflammatory infiltrate is typically lymphocytic in nature, with admixed histiocytes. The inflammation is primarily centered on myocytes, although interstitium may be involved. Varying extent of inflammation of the endocardial and epicardial fat maybe present. Necrosis is present but is milder in extent when compared to the degree of inflammation. The degree of infiltration may be especially marked in infants and young children, and there may be scattered neutrophils and histiocytes, in addition to lymphocytes.
Endomyocardial biopsies (EMB) are often performed in clinically suspected cases of myocarditis, but these have a low diagnostic yield owing to sampling issues. The World Health Organization and International Society and Federation of Cardiology Task Force define myocarditis as an inflammatory disease of the myocardium diagnosed by histological (Dallas criteria), immunological, and immunohistochemical criteria. The Dallas Criteria requires the presence of an inflammatory infiltrate and myocyte necrosis of nonischemic origin. The myocyte alterations are best appreciated in longitudinal sections and can include range of changes from myocyte vacuolization, myocyte disruption, degenerated cytoplasm, lack of cross striations, intracytoplasmic lymphocytes, to frank necrosis.
However, these criteria are subject to high degree of interobserver variability and are poor predictors of response to immunosuppressive therapy. For these reasons, it is recommended that on biopsy specimens, the diagnosis of myocarditis be made with any degree of significant inflammation. It is also recommended that fibrosis, when present, be scored on both a quantitative (mild, moderate, and severe) and qualitative (interstitial, endocardial, and replacement) scale. Subsequent follow-up biopsies need to be graded in comparison to the index biopsy, as ongoing/persistent myocarditis (if myocyte damage and inflammation persists), resolving myocarditis (if the changes are reduced), and healed myocarditis if the changes completely resolve. For the diagnosis of myocarditis, at least three endomyocardial samples need to be collected for light microscopy. Additional samples should be snap frozen in liquid nitrogen for viral polymerase chain reaction studies. The immunohistochemical criteria that is suggested for diagnosing myocarditis includes, >14 WBCs/mm2, including up to 4 monocytes/mm2 with the presence of CD3 positive T-lymphocytes >7 cells/mm2.
In autopsy specimens, the significance of finding of focal myocardial inflammation (<5 microscopic foci) in the absence of a clinical correlate has been subject of debate. It has been suggested that focal inflammation with or without necrosis, is more likely to be encountered in deceased individuals on antibiotics.
Catecholamine-induced myocardial injury shows contraction band necrosis and disproportionately sparse inflammation. “Contraction bands” represent hypercontracted myocytes in which transverse bands of condensed myofilaments are visible on light microscopy. In contraction band necrosis, there is necrosis of single cells or a small cluster of cells with associated mononuclear infiltrate. Contraction band necrosis can be seen in patients with reperfusion infarction and cerebral hypoxia patients maintained on pressors. This may also be seen in patients with exogenous use of catecholamines or related drugs of abuse. In this respect, catecholamine-induced myocarditis represents an example of toxic myocarditis, an etiologic designation corresponding to dose related myocardial inflammation caused by a drug or exogenous toxic agent. Toxic myocarditis is due to direct myocyte injury (rather than immune mediated) and generally persists despite cessation of the drug.
Hypersensitivity myocarditis is most often an incidental finding detected in autopsy hearts, explanted hearts, and in left ventricular cores removed at the time of assist device placement. These represent a delayed hypersensitivity reaction to a drug and are therefore mechanistically different from toxic myocarditis. A specific etiologic agent is rarely identified. A variety of drugs have been implicated including antibiotics, metoprolol, sulfasalazine, anti-tuberculous drugs, herbal supplements, and adalimumab.
The term "eosinophilic myocarditis" is often used for symptomatic patients; etiologies include hypersensitivity myocarditis, Churg-Strauss syndrome, parasitic infections, and chronic eosinophilic leukemia. Patients present with signs and symptoms of myocarditis and cardiac failure with or without skin rash. Symptoms occur within weeks of exposure to an agent and generally resolve with removal of the offending agent. Histologically, eosinophilic myocarditis and hypersensitivity myocarditis are similar and show an interstitial and perivascular infiltrate of macrophages, lymphocytes, eosinophils, and mast cells. Small poorly formed granulomas may occur. In symptomatic eosinophilic myocarditis, there is diffuse inflammatory infiltrate of eosinophils with necrosis.
Giant cell myocarditis (Fiedler myocarditis, GCM) is a rare disorder of uncertain etiology, which is presumed to be an autoimmune condition. Patients with GCM have associated autoimmune disorders in up to 8% of cases. GCM affects young to middle-aged adults with a slight predilection for males. Most patients follow a rapidly progressive course from congestive failure to cardiogenic shock that is unresponsive to conventional treatments. GCM patients are more likely to present as ventricular tachycardia and/or sudden cardiac death. Gross findings include cardiomegaly with diffuse, poorly demarcated areas of yellow-brown discoloration. Rarely mural thrombi and ventricular wall rupture may be seen. Histologically, there is diffuse infiltration of the myocardium by a mixture of abundant lymphocytes (predominantly CD8(+), T-cells), some eosinophils and plasma cells, and many scattered giant cells. The giant cells are Langhans type multinucleated macrophage giant cells that are involved in phagocytosis of necrotic myocytes. These are commonly found at the interface between the normal myocardium and active lesions and may demonstrate intracytoplasmic degenerated myocyte fibers. In early stages of the GCM, myocyte necrosis is invariably seen. As the disease progresses, there is varying degree of granulation tissue formation, collagen deposition, and fibrosis. In the later stages of the disease, giant cells are increasingly difficult to find.
In contrast, in cardiac sarcoidosis, the giant cells are found in association with well-formed granulomas. With sarcoidosis, it is uncommon to find myocyte necrosis and eosinophils, while fibrosis tends to be robust. GCM needs to be aggressively managed with corticosteroids and calcineurin inhibitors.
Supplementary Questions
- Which of the following is the most common infectious etiology for myocarditis in North America?
- Coxsackie virus
- Cytomegalovirus
- Hepatitis C virus
- Mycobacterium tuberculosis
- Toxoplasma
- Which of the following conditions is associated with prominent contraction band necrosis?
- Catecholamine-induced injury
- Eosinophilic myocarditis
- Giant cell myocarditis
- Lymphocytic myocarditis
- Sarcoidosis
- Which of the statements regarding giant cell myocarditis (GCM) is true?
- GCM is a potentially fatal condition and needs to be managed aggressively.
- GCM is an incidental finding seen in left ventricular cores of patients on a cardiac transplant wait list.
- GCM shows well-formed, tight granulomas with giant cells.
- Necrosis is not a common histological feature.
- The majority of the giant cells in GCM are of myocyte origin.
References
- Cardiomyopathy and Myocarditis. In: Rosai J (ed). Rosai and Ackerman’s Surgical Pathology – 10th ed. Mosby Elsevier; 2011:2271-2282.
- Burke AP, Alexiev B, Aubry MC, Joseph Maleszewski J, Tavora JF (eds). Practical Thoracic Pathology: Diseases of the Lung, Heart, and Thymus. Philadelphia, PA; Wolters Kluwer;2017.
- Caforio ALP, Pankuweit S, Arbustini E, et al. European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34(33):2636-2648.
- Fronczek J, van de Goot FRW, Krijnen PAJ, van der Wal AC, Niessen HWM. Diagnosing lymphocytic myocarditis in adult autopsies combining the Dallas criteria with immunohistochemical stainings. J Forensic Res. 2016;325: doi:10.4172/2157-7145.1000325
- Kang M, An J. Myocarditis, Viral. [Updated 2017 Oct 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2017 Jun. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459259/
Author
Vijayalakshmi Ananthanarayanan, MBBS, MD, FCAP
Surgical Pathology Committee
Loyola University Medical Center
Maywood, IL
Answer Key
- Coxsackie virus (a)
- Catecholamine-induced injury (a)
- GCM is a potentially fatal condition and needs to be managed aggressively. (a)