Clinical Summary
A 50-year-old man presents with longstanding hematuria and flank pain, and a 9.5 x 8.5 x 6.8 cm right renal mass with retroperitoneal lymphadenopathy is identified on computed tomography scan. The patient undergoes radical nephrectomy, where a similarly sized white-tan firm renal mass is found invading the pelvicalyceal system, renal sinus, and perinephric tissue, with a renal vein thrombosis. A total of 34 out of 45 regional lymph nodes are involved by metastatic tumor. The adrenal gland is present and uninvolved. On immunohistochemistry, the tumor cells are negative for multiple keratins and melanocytic markers. Tumor cells mark with CD10, P504S, TFE3, and CA-IX.
Master List of Diagnoses
- Clear cell papillary renal cell carcinoma
- Clear cell renal cell carcinoma
- Multilocular cystic renal cell neoplasm of low malignant potential
- Papillary renal cell carcinoma
- TFE3-associated renal cell carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology 2019, Case 04, and is TFE3-associated renal cell carcinoma (kidney).
Criteria for Diagnosis and Comments
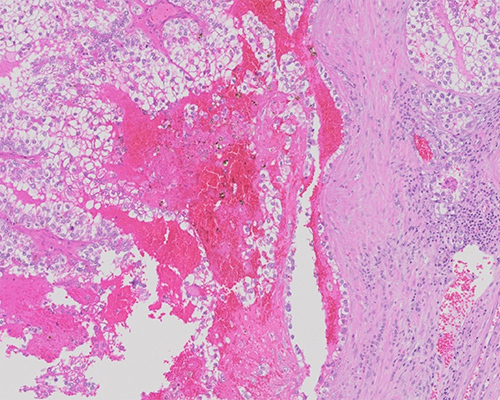
Histologic sections show a fairly well-defined, non-encapsulated renal mass with variably solid/nested and papillary architecture with focal necrosis and hemorrhage. Tumor cells have discrete/defined cell borders and abundant clear to eosinophilic flocculent cytoplasm. Nuclei are relatively uniform, with vesicular chromatin and nucleoli visible at 10x. Psammoma bodies are variably present. Based on the morphology and immunoprofile, this tumor is classified as a TFE3-associated renal cell carcinoma (RCC).
The Microphthalmia-TFE (MiT) translocation renal cell carcinoma family is composed of 2 members: TFE3-associated RCC (involving Xp11 translocations) and TFEB-associated RCC (involving t(6;11)). The TFE3-associated RCCs were first recognized in the 2004 World Health Organization (WHO) classification as Xp11 translocation RCC. They were reclassified in the 2016 WHO classification along with t(6;11) RCCs under the broader heading of MiT family translocation RCC. Approximately 20% to 75% of pediatric RCCs are TFE3-associated RCCs. Only 1.6% to 4% of adult RCC are TFE3-associated and fewer than 100 cases have been reported in the literature.
TFE3-associated RCCs harbor fusions of TFE3 with a variety of gene partners, all of which act as promoters to upregulate TFE3 expression from constitutively low levels to levels detectable by immunohistochemistry. The most common partner is PRCC, resulting from t(X;1)(p11.3;q21). The second-most common partner is ASPL (also called ASPSCR1), resulting from t(X;17)(p11.2;q25), the same fusion gene in alveolar soft part sarcoma. Other recurrent partners include NONO, SFPQ, CLTC, and RBM10. TFEB-associated RCCs result from t(6;11), which fuses TFEB with MALAT1, a gene which is transcribed into a non-coding ribonucleic acid of unknown function. When overexpressed, TFE3 and TFEB each act as aberrant transcription factors that activate a variety of downstream targets, many of which are normally activated by other MiT family members (such as cathepsin K).
Microscopically, TFE3-associated RCC are composed of papillary or nested epithelioid tumor cells with ample clear to eosinophilic cytoplasm, distinct cell borders, and abundant psammoma bodies. The morphology of PRCC-TFE3 RCC differs from ASPL-TFE3 RCC: PRCC fusions always show a nested (solid, alveolar, acinar, or tubular) pattern with foci of papillary architecture with less abundant cytoplasm and fewer psammoma bodies as compared with ASPL. However, these morphologic differences are not sufficiently distinct to rely on H&E assessment alone for genetic classification. Some TFE3-associated RCC show melanin pigment (the so-called “melanotic translocation RCC,” including fusion partners SFPQ and ARID1B), creating overlap between TFE3-associated RCC and TFE3-associated PEComas. The SFPQ-TFE3 tumors have a distinctive morphology of subnuclear vacuoles and nuclear palisading, similar to that seen in endometrium.
Overall, TFE3-associated RCCs show high-grade features (necrosis and renal parenchymal invasion). Depending on the elements present, TFE3-associated tumors may mimic clear cell RCC, papillary RCC, clear cell papillary RCC, or multilocular cystic renal neoplasm of low malignant potential. TFEB-associated RCC, in contrast, are biphasic with nests of larger periepithelioid cells and smaller cells clustered around basement membrane material. Entrapped single renal tubules are found at the tumor edge.
In contrast to other RCC, the MiT family of translocation-associated RCC under expresses cytokeratins and epithelial membrane antigens but still consistently expresses PAX8 and other markers of renal tubular origin. The melanotic translocation RCC subgroup expresses melanocytic markers and will show intracytoplasmic melanin pigment. The t(6;11) tumors consistently express Melan-A, HMB45 and cathepsin K, which are also expressed in TFE3-associated RCCs to a lesser degree (60% labeling for cathepsin K, which is likely dependent on the fusion partner, with PRCC-TFE3 fusion tumors having higher rates of expression than ASPL-TFE3 fusion tumors). Diagnosis is by reverse transcriptase- polymerase chain reaction (PCR), immunohistochemistry using an antibody to the C-terminus of TFE3 or an antibody for the TFEB protein, or fluorescence in situ hybridization (FISH) using TFE3 or TFEB break-apart assays, which are the preferred methods as FISH is less susceptible to fixation issues and antibody incubation times.
Survival for patients with TFE3-associated RCC is comparable to those with clear cell RCC and significantly worse than that for patients with papillary RCC. Within the TFE3-associated RCC, however, there remains tremendous variability in survival rates, which is hypothesized to be related to the fusion partner. Fusions with ASPL result in tumors with more regional lymph node metastasis; however, most of these node-positive patients remain disease-free without adjuvant therapy. TFEB-associated RCC are considered more indolent than the TFE3-associated tumors, with a potential for late metastasis 20-30 years after initial diagnosis.
Clear cell renal cell carcinoma (ccRCC) is a morphologically heterogeneous group accounting for 65% to 70% of all renal cancers. While the majority of ccRCC occur sporadically, several familial syndromes give rise to them, including von Hippel-Lindau, Cowden, and Birt-Hogg-Dube syndromes, tuberous sclerosis, and succinate dehydrogenase-deficient renal cell carcinoma syndrome. In sporadic and VHL cases alike, these tumors have a classic vascular pattern related to inactivation of VHL on 3p25 and upregulation of hypoxia-inducible factor alpha. ccRCC are architecturally diverse and include solid alveolar patterns, most commonly with a network of delicate vessels. Tumor cell cytoplasm is filled with lipids and glycogen which dissolve during processing, resulting in the so-called “clear cell” appearance, but many show eosinophilic cytoplasm, particularly high-grade tumors and areas adjacent to necrosis or hemorrhage. ccRCC may express AE1/3, CAM5.2, and/or EMA, but CK7 expression is rare and limited. ccRCC also express PAX8 and CA-IX. CD10 and vimentin are also expressed but are nonspecific.
Multilocular cystic renal neoplasm of low malignant potential (formerly multilocular cystic renal cell carcinoma) accounts for fewer than 1% of all renal tumors and is usually discovered incidentally. Tumors consist of variably sized cysts separated by thin septa containing scattered tumor cells. Multilocular cystic renal neoplasm of low malignant potential is not a diagnostic consideration once mural nodules of tumor are identified. Tumor cells have ample clear cytoplasm with International Society of Urologic Pathology (ISUP) grade 1 to 2 nucleoli and are found lining the cyst walls and in small quantities within the septae. Necrosis, vascular invasion, and sarcomatoid features are also incompatible with the diagnosis. VHL mutations have been found in 25% of tumors, and chromosome 3p deletion has been found in 74%. Using strict criteria, no tumor has ever been found to recur or metastasize.
Papillary renal cell carcinoma (PRCC) is the second-most common RCC after ccRCC, with a wide age range. In the pediatric group, PRCC are proportionately more common than in adults, where it is associated with end-stage renal disease or acquired cystic renal disease. There is a familial PRCC syndrome with a high degree of penetrance, and tumors are also part of the Birt-Hogg-Dube syndrome.
PRCC is more likely than ccRCC to show necrosis and undergo spontaneous hemorrhage, and up to 30% of cases show calcifications. Morphologically, tumors are well-circumscribed and composed of papillae formed by delicate fibrovascular cores with foamy macrophages and psammoma bodies. Morphology is variable, from tubular to a packed, solid appearance.
Tumors have historically been divided into Type I and Type II tumors, and although Type II tumors may actually represent a heterogeneous group, the designation can still be helpful. Type I tumors have papillae covered with a single layer of cells with scant, pale cytoplasm, while Type II tumors show nuclear stratification and higher nuclear grade, with more eosinophilic cells. A third category, oncocytoma-like PRCC, has not been fully characterized. Tumor cells express AE1/3, CAM 5.2, HMWK, EMA, and others, similar to ccRCC. CK7 expression is more common in Type I PRCC than Type II. Tumors show trisomy/tetrasomy 7 and trisomy 17, and loss of Y. Spread is similar to ccRCC (vascular).
Clear cell papillary renal cell carcinoma is an indolent tumor accounting for 1% to 4% of all renal tumors. It arises in the setting of end-stage renal disease and von Hippel-Lindau syndrome but is most frequently detected incidentally. Tumor morphology is variable, with tubular, papillary, acinar, cystic, ribbon-like, and solid patterns. Other patterns include a collapsed acinar-like pattern, or solid pattern. The vascular network is delicate, similar to ccRCC. Tumor cells are cuboidal to low-columnar, with characteristic uniform palisading ISUP grade 1 to 2 nuclei oriented away from the basal aspect of the cells. Apical snouts may be seen. Tumor necrosis, perirenal invasion, and lymphovascular invasion are absent. Tumor cells express CK7 diffusely and mark with PAX2 and PAX8. CA-IX characteristically stains cells in a so-called “cup-like” pattern.
Supplementary Questions
- Which of the following statements is true regarding TFE3-associated renal cell carcinomas (RCC)?
- Generally speaking, they do not have necrosis or other high-grade features.
- Their spread is primarily lymphatic.
- They are less aggressive than TFEB RCC.
- They may mimic clear cell RCC.
- They show morphologic, immunophenotypic, and behavioral uniformity.
- Which of the following statements is true regarding TFE3 fusion tumors?
- ASPL fusion tumors are part of the melanotic translocation RCC family.
- ASPL fusion tumors show fewer regional lymph node metastases than PRCC fusion tumors.
- PRCC fusion tumors show more psammoma bodies than ASPL fusion tumors.
- PRCC fusion tumors show higher rates of cathepsin K expression than ASPL fusion tumors.
- TFE3 fusion partners include PRCC, ASPL, SFPQ, and MALAT1.
- Which of the following statements is true regarding ancillary testing for TFE3-associated tumors (immunohistochemistry, polymerase chain reaction [PCR], and fluorescence in situ hybridization [FISH])?
- FISH using a TFE3 fusion probe is the preferred test due to lack of issues with fixation and/or incubation times.
- Reverse transcriptase PCR is an unreliable method of diagnosing TFE3 RCCs.
- TFE3 immunophenotype is variable and depends on the fusion partner.
- TFE3 immunostain consistently detects expression in TFE3 tumors and is the test of choice for diagnosis.
- TFE3 RCCs consistently express Melan A, HMB45, and cathepsin K.
References
- Antic T, Taxy JB, Alikhan M, Segal J. Melanotic Translocation Renal Cell Carcinoma with a Novel ARID1B-TFE3 Gene Fusion.” Am J Surg Path. 2017;41(11):1576-1580.
- Moch H, Humphrey PA, Ulbright TM, Reuter VE, eds. WHO Classification of Tumours of the Urinary System and Male Genital Organs. International Agency for Research on Cancer. 2016;18-40.
- Want XT, Xia QY, Ni H, et al. SFPQ/PSF-TFE3 renal cell carcinoma: a clinicopathologic study emphasizing extended morphology and reviewing the differences between SFPQ-TFE3 RCC and the corresponding mesenchymal neoplasm despite an identical gene fusion. Hum Path. 2017;63:190-200.
- Xia QY, Wang Z, Chen N, et al. Xp11.2 translocation renal cell carcinoma with NONO-TFE3 gene fusion: morphology, prognosis, and potential pitfall in detecting TFE3 gene rearrangement. Mod Path. 2017; 30(3):416-426.
- Xiong L, Chen X, Liu N, et al. PRCC-TFE3 dual-fusion FISH assay: A new method for identifying PRCC-TFE3 renal cell carcinoma in paraffin-embedded tissue. PLoS, published online 2017. https://doi.org/10.1371/journal.pone.0185337; Accessed November 8, 2018.
Author
Sabrina C. Sopha, MD, FCAP
Surgical Pathology Committee
University of Maryland Baltimore Washington Medical Center
Answer Key
- They may mimic clear cell RCC. (d)
- PRCC fusion tumors show higher rates of cathepsin K expression than ASPL fusion tumors. (d)
- TFE3 immunophenotype is variable and depends on the fusion partner. (c)