Clinical Summary
A 70-year-old man presents with vague abdominal pain and increasing jaundice. His past medical history is notable for chronic hepatitis C. A computed tomography scan reveals a left lobe mass in the liver. Gross examination of the hepatic lobectomy specimen reveals a cirrhotic liver with a tan soft 9 cm mass. Of note, the gallbladder and extrahepatic bile ducts are unremarkable on gross examination and histologically.
Master List of Diagnoses
- Dysplastic nodule
- Focal nodular hyperplasia
- Hepatocellular carcinoma
- Intrahepatic cholangiocarcinoma
- Macroregenerative cirrhotic nodule
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 05, and is hepatocellular carcinoma (liver).
Criteria for Diagnosis and Comments
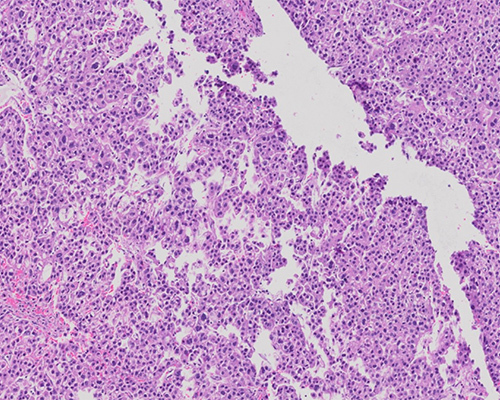
The histological sections demonstrate a circumscribed hepatic lesion comprised of sheets and trabeculae of polygonal neoplastic cells with eosinophilic granular cytoplasm. The tumor cells nuclei demonstrate marked atypia, ie, hyperchromasia, multinucleation, increased nucleus to cytoplasm ratio, and irregular nuclear membranes. There are clusters of neoplastic cells that demonstrate clear cytoplasm and others that form pseudoglands. Foci of vascular invasion are present. These features are those of hepatocellular carcinoma in a cirrhotic background.
Hepatocellular carcinoma (HCC) is the most common primary hepatic malignancy. It is the third leading cause of cancer-related deaths in the world however it is less common in the United States where it is frequently seen in men and African Americans. China and Japan have the highest rates of HCC. The incidence is also high in developing countries and continues to rise in industrialized nations.
The majority of HCC arise in the background of chronic liver disease, with chronic viral hepatitis B and hepatitis C accounting for 80% of cases. Alcohol- and non-alcohol-related fatty liver disease, as well as tobacco use and increasing age, are also etiological factors. The ingestion of aflatoxin is linked to HCC in Asian and sub-Saharan African nations. Chronic liver injury due to hereditary factors like hemochromatosis and α-1 antitrypsin deficiency increases the risk of HCC, while patients with inherited metabolic diseases, such as glycogen storage disease, also have higher risk of developing HCC. Lastly, HCC could develop from some variants of hepatic adenomas in the absence of chronic liver disease. The coexistence of multiple risk factors significantly increases the risk of cirrhosis which, independent of etiology, is a major clinical risk factor for the development of HCC.
Grossly, HCC can be solitary or multiple. Oftentimes, a dominant nodule will be associated with smaller satellite lesions. A fibrous capsule separating the tumor from the surrounding stroma may be present.
Many grading systems exist for HCC, including the Edmondson and Steiner system, which divides the tumors into 4 grades from I to IV based on histological differentiation:
- Grade I: Tumor cells with abundant cytoplasm and minimal nuclear atypia
- Grade II: Mild nuclear atypia with prominent nucleoli, hyperchromasia, and nuclear irregularity
- Grade III: Moderate nuclear atypia with greater hyperchromasia and nuclear irregularity
- Grade IV: Marked nuclear pleomorphism, marked hyperchromasia, and anaplastic giant cells
Most HCC are either grade II or III. It should be noted that tumor grade is not a strong prognostic factor. Many experts instead prefer a simpler classification of well, moderately, and poorly differentiated tumor.
There is variation in both the architectural growth patterns and the degree of cytologic atypia. Neoplastic cells have abundant to moderate amounts of cytoplasm, which can be pink with Mallory hyaline and show fatty or clear cell change. Large round nuclei and prominent nucleoli are common. Solid, trabecular, and pseudoglandular growth patterns are frequently encountered. There is loss of the normal hepatic plate structure, as can be observed with the help of a reticulin stain. The presence of arteries unaccompanied by portal tracts is a common feature of HCC.
HCC are often easily recognized on routine H&E staining; however, histochemical and immunostains are helpful when the diagnosis is difficult. Diffuse expansion and/or loss of reticulin staining are frequent in hepatocellular carcinoma. CAM5.2 is positive in all HCC. CD10 and polyclonal carcinoembryonic antigen (pCEA) are expressed by up to 90% of HCC in a canalicular pattern. CD34 shows a strong diffuse sinusoidal staining pattern in HCC. HepPar1 has shown increased sensitivity for well to moderately differentiated HCC. Glypican 3 labels up to 85% of HCC and does not stain a non-inflamed and non-cirrhotic background liver. Overall, it is best to use a panel of markers when the diagnosis is in doubt, including arginase-1, a specific and sensitive marker for benign and malignant hepatocytes.
Some HCC may arise in the absence of cirrhosis, one such example being fibrolamellar HCC. This subtype is rare and encountered in younger patients than conventional HCC. Grossly and histologically, the presence of fibrous septae, similar but more diffuse than the septae of focal nodular hyperplasia, is the hallmark of this neoplasm. Tumor cells grow in trabeculae between these septae. The neoplastic cells have very eosinophilic cytoplasm with frequent pale inclusions and cytoplasmic globules. These tumors can show CK7 and CK19 labelling. They have traditionally been thought to have a better prognosis than conventional HCC due to the absence of background cirrhosis, but recent evidence suggests that this tumor could be biologically similar or more aggressive than conventional HCC with early invasion into major hepatic vessels.
In the absence of screening programs, HCC is often diagnosed late in its course, and the median survival following diagnosis is approximately 6 to 20 months. Surgical resection is the mainstay of treatment; however, resection may not be possible due to the extent of underlying liver disease. For these patients, along with those meeting the Milan criteria (ie, a single tumor ≤ 5.0 cm in diameter or up to three separate lesions, none of which is larger than 3.0 cm, no evidence of gross vascular invasion, and no regional nodal or distant metastases), liver transplantation is an option. To decrease the size and/or number of tumors, patients are often treated with radiofrequency ablation, transarterial chemoembolization, cryoablation, systemic chemotherapy, or stereotactic radiotherapy.
For tumors confined to the liver, the five-year survival rate is 28%. Tumors with regional spread (growth into nearby organs), the five-year survival rate is 7%. Once distant metastases develop, survival time is as low as two years. Tumors that have been completely surgically removed and those that are diagnosed early may have a five-year survival rate as high as 50% to 70%.
Dysplastic nodules can be single or multiple. They are more commonly associated with cirrhotic livers but have been noted in chronic liver disease without significant fibrosis. Dysplastic nodules range from 0.5 to 5.0 cm in size and are associated with higher risk of development of hepatocellular carcinoma. Grossly, dysplastic nodules differ from the background liver in their color, size, texture, and a degree of bulging on cut surface. The hepatic plates can be up to 2 cells thick. Dysplasia within these lesions is classified as low- and high-grade. Low-grade dysplasia is characterized by mild increase in cellularity of a monotonous cell population without significant architectural atypia. Portal tracts are present within the nodule.
Large cell change, defined as cellular enlargement, nuclear pleomorphism and hyperchromasia, and multinucleation of hepatocytes, used to be regarded as a feature of low-grade dysplasia, but is now recognized as evidence of replicative senescence rather than a premalignant lesion. Low-grade dysplastic nodules are not easily distinguished from large macroregenerative nodules. The presence of arteries unpaired with bile ducts and a clone-like cell population favors dysplasia. High-grade dysplasia is characterized by small cell change, which has been described as a collection of hepatocytes with a decreased cell volume, minimal nuclear pleomorphism, an increased nucleus to cytoplasm ratio, and an increased nuclear density.
Macroregenerative cirrhotic nodules are collections of regenerative hepatocytes arising in a background of cirrhosis. There can be multiple nodules in a cirrhotic liver. They are slightly larger than the background liver nodules and vary in size from 1 to 5 cm. Hepatic plates are mildly thickened, 1 to 2 cells thick. Scattered entrapped portal tracts are present within the nodule. The hepatocytes within the nodule resemble those in the adjacent liver parenchyma. Mallory hyaline, foci of bile ductular reaction, and inflammation can be present within a macroregenerative nodule.
Intrahepatic cholangiocarcinoma (ICC) is an intrahepatic malignancy with biliary epithelial differentiation. It comprises 10% of primary liver malignancies. Any portion of the intrahepatic biliary network can give rise to this tumor. The age-specific incidence is highest in patients over 85 years. It is more commonly encountered in men and in Southeast Asian countries. Biliary and hepatic diseases such as primary sclerosing cholangitis, hepatolithiasis, parasitic infection of the biliary tract (liver flukes Clonorchis sinensis or Opisthorchis viverrini), biliary malformations, and non-biliary causes of cirrhosis (eg, viral hepatitis) are all risk factors for ICC. In addition, exposure to Thorotrast has also been associated with the development of ICC.
ICC can arise in association with biliary intraepithelial neoplasia (BilIN). The majority of ICC are adenocarcinomas. The cells are columnar/cuboidal and form variably sized tubular structures that resemble bile ducts forming acinar, cord-like or papillary patterns of growth. The nuclei are round and centrally located. The glands are surrounded by acellular fibrous stroma with variable amounts of inflammation. Adenosquamous, squamous, clear cell, signet ring cell, lymphoepithelioma-like, mucinous, and sarcomatous histologic variants have been described. Mucin stains (mucicarmine, diastase-periodic acid Schiff, alcian blue) are positive in the tumor. CK7 and CK19 are often expressed by the neoplastic cells as are carcinoembryonic antigen and epithelial membrane antigen. ICC is an aggressive cancer that carries a poor prognosis and typically spreads by direct invasion, along hepatic plates and nerves.
Focal nodular hyperplasia is a benign condition that develops as a result of shunting of arterial blood flow which leads to the production of fibrous bands. It is a benign and non-neoplastic condition. Histologically, the lesion is comprised of nodules of benign hepatocytes with intervening thin fibrous septae. The reticulin staining pattern demonstrates normal-thickness (1 - 2 cells) hepatocyte trabeculae. Ductular reaction can be seen in the fibrous septae. The background liver is non-cirrhotic and glutamine synthetase immunostain demonstrates map-like staining.
Supplementary Questions
- Which of the following is correct regarding hepatocellular carcinoma (HCC) in the United States?
- Clonorchis sinensis and Opisthorchis viverrini infection are important risk factors.
- HCC are more frequently encountered in men and in African Americans.
- Portal tracts are readily identified within the tumor.
- The lesion develops as result of shunting of arterial blood flow, which leads to the production of fibrous bands around nodules of hepatocytes.
- Tumor grade is a strong prognostic factor.
- Which of the following is correct of the fibrolamellar variant of hepatocellular carcinoma?
- Neoplastic cells with eosinophilic cytoplasm with frequent pale inclusions and cytoplasmic globules grow between dense fibrous septae.
- Small cell change is a prominent feature.
- The tumor is distinguished by CK7- and CK19-positive glands of cuboidal cells embedded in fibrotic stroma.
- The tumor is comprised of regenerative hepatocytes arising in a background of cirrhosis with no expansion of the hepatic plates.
- The tumor is the result of shunting of arterial blood flow, which leads to the production of fibrous bands.
- Which of the following are histologic features of a dysplastic hepatic nodule?
- Collections of hepatocytes with a decreased cell volume, minimal nuclear pleomorphism, an increased nucleus to cytoplasm ratio, and increased nuclear density
- Entrapped portal tracts with hepatocytes sharing the same histologic features as those in adjacent parenchyma
- Expanded and disrupted hepatic plate architecture with neoplastic cells growing in solid, trabecular, and pseudoglandular patterns
- Marked nuclear pleomorphism, marked hyperchromasia, and anaplastic giant cells
- Nodular expansion of hepatocytes with intervening thin fibrous septae
References
- Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer. 1954;7(3):462-503.
- Paradis V. Histopathology of Hepatocellular Carcinoma. Recent Results Cancer Res. 2013;190:21-32.
- Schlageter M, Terracciano ML, D’Angelo S, Sorrentin P. Histopathology of hepatocellular carcinoma. World J Gastroenterol. 2014; 20(43):15955–15964.
Author
Safia N. Salaria, MD
Surgical Pathology Committee
Vanderbilt University Medical Center
Nashville, TN
Answer Key
- HCC are more frequently encountered in males and in African Americans. (b)
- Neoplastic cells with eosinophilic cytoplasm with frequent pale inclusions and cytoplasmic globules grow between dense fibrous septae. (a)
- Collections of hepatocytes with a decreased cell volume, minimal nuclear pleomorphism, an increased nucleus to cytoplasm ratio, and increased nuclear density (a)