Clinical Summary
A 63-year-old woman presents with abdominal pain and swelling of several weeks’ duration. Radiologic imaging reveals an 11 cm centrally placed heterogenous mass in the liver. The resected liver demonstrates a gray-white, variegated, and poorly circumscribed mass with foci of necrosis, cystic change and alternating firm and soft solid areas within the tumor. The tumor is largely intrahepatic but attached to the wall of the IVC, partially occluding the hepatic veins. Immunohistochemically, the tumor cells are positive for vimentin, alpha smooth muscle actin (SMA), and h-caldesmon; weak focal staining for S100 and CD34 is also noted, but desmin, ERG-1, CD117/c-KIT, DOG-1, EMA, CK18, and cytokeratin AE1/3 are negative.
Master List of Diagnoses
- Angiosarcoma
- Gastrointestinal stromal tumor
- Leiomyosarcoma
- Monophasic synovial sarcoma
- Sarcomatoid hepatocellular carcinoma
- Solitary fibrous tumor
- Undifferentiated embryonal sarcoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 16, and is leiomyosarcoma in the liver.
Criteria for Diagnosis and Comments
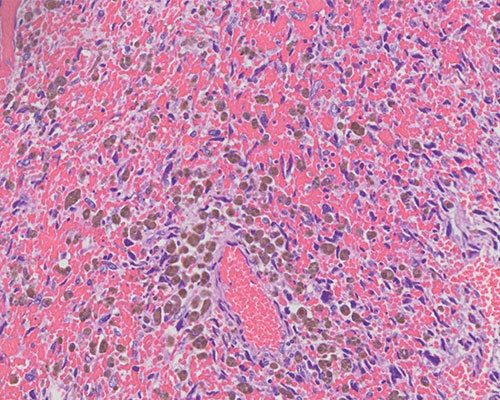
The histological sections from this tumor demonstrate a spindle cell neoplasm arranged in fascicles. The neoplastic cells have round to oval to elongated nuclei, and mitoses are present, focally, with as many as 5 per high-power field. Some sections show extreme nuclear pleomorphism, but the majority of the lesion has little of this feature. By immunohistochemistry, the lesion demonstrates smooth muscle phenotype being positive for SMA, calponin, and h-caldesmon, although negative for desmin, which can occur in a minority of leiomyosarcoma (LMS). In addition, the lesional cells do not react with endothelial markers (ERG-1, Claudin5), gastrointestinal stromal tumor markers (CD117/c-KIT, DOG-1), or epithelial markers (EMA, CK18, CKAE1/3). Lastly, focal/weak positivity for S100 and CD34 is compatible with LMS, which is the correct diagnosis for this case.
Hepatic leiomyosarcoma (hLMS) is very rare and likely to originate from the ligamentum teres or from the wall of an intrahepatic vessel. However, many cases of LMS involving the liver originate from the wall of the retrohepatic IVC, extending from there into the liver. LMS could also metastasize to the liver. LMS represents less than 1% of all liver malignancies. LMS of the liver occurs in older patients with a mean age of 58 years, but occurrence in much younger patients has also been reported. Presentation depends on the size and site and includes Budd-Chiari syndrome in patients having IVC/hepatic vein involvement, palpable (or visible) abdominal mass, upper abdominal pain or heaviness, weight loss, early satiety, and others.
Ultrasound, computed tomography (CT) scan and magnetic resonance imaging (MRI) have been utilized in the diagnosis of hLMS. With CT, primary hLMS is usually a single heterogeneous, hypodense, and hypervascular mass, with internal and peripheral enhancement, or occasionally a cystic mass with an enhancing thick wall. The enhancement patterns vary, with larger tumors enhancing conspicuously on hepatic arterial phase. The enhancement type could be similar to hepatocellular carcinoma (HCC), but in contrast to HCC, LMS is more hypervascular and may demonstrate isodensity both on portal venous and hepatic parenchymal phases. Other authors have recommended MRI with contrast-enhanced MR venography specifically when clinical considerations include IVC LMS, since this modality is able to distinguish the tumor from thrombus of the IVC in addition to defining its size and other parameters.
Surgery is the mainstay of management with or without neoadjuvant chemotherapy. When necessary, to achieve adequate post-operative residual liver volume, pre-operative portal vein embolization could be performed to cause atrophy of the lobes of liver to be resected and stimulate compensatory hyperplasia/hypertrophy of the remaining lobe(s).
Routine and immunohistochemical characteristics are fairly straightforward in diagnosing LMS at most sites including the liver or IVC. Except in very poorly differentiated cases with large pleomorphic cells, most LMS show some evidence of smooth muscle differentiation. These include spindle cells with so-called cigar-shaped nuclei; cytoplasmic vacuoles, often at the ends of these nuclei; and fascicular arrangement. Depending on the site of origin, the differentiation between low-grade/well-differentiated LMS and benign leiomyoma could be difficult. However, in the liver (or IVC), this problem rarely exists since the required 1-2 mitoses per 10 high-power fields and/or large tumor size and/or presence of necrosis to make the diagnosis of LMS are almost always present.
The less-differentiated patterns, including epithelioid, rhabdoid, pleomorphic, and myxoid variants, have rarely been reported at this site. Irrespective of the degree of differentiation, LMS typically expresses more than one smooth muscle marker including SMA, calponin, h-caldesmon, and desmin. H-caldesmon has been regarded as the most specific marker for muscle differentiation among this list, being negative in myofibroblastic lesions and some other sarcomas that could focally express one or more smooth muscle markers. Most LMS are S100 negative, but focal staining with this marker, as well as with CD34, has been reported.
Angiosarcoma (AS) are commonly multifocal lesions in the liver and rarely grow to the size seen in this case. AS could range from vasoformative (well-differentiated) to epithelioid and/or solid lesions. Tumor cells are very atypical and hobnail into vascular channels when present. Cytoplasmic lumina containing red cells could be seen, while solid and predominantly epithelioid variants could demonstrate no apparent evidence of endothelial differentiation without immunohistochemistry. Immunohistochemically, AS reacts with endothelial markers and expression of at least 2 of these (for example, CD31, CD34, ERG-1, claudin5, and factor VIII-related antigen) is required for diagnosis of AS. In the current case, negative ERG-1 and claudin5, despite focal/weak CD34, in addition to positive muscle markers, clearly exclude AS.
Gastrointestinal stromal tumor (GIST) and solitary fibrous tumor (SFT) could rarely present in the liver as primary diseases. Both of these lesions are characterized by positive CD34 lesional cells. The degree of cellularity and atypia in the presented case, as well as its growth pattern into the wall of the IVC, would be totally unusual for SFT, which is almost always benign. However, a case of malignant SFT involving the liver has been described with features that overlapped with LMS; but even then, malignant SFT rarely expresses smooth muscle markers to the extent seen with LMS, and it does express STAT6. GIST can be spindled or predominantly epithelioid and reacts positively for CD117/c-KIT and DOG-1, which is not the case in this patient.
Monophasic synovial sarcoma (SS) originating in the liver, though rare, has been reported. Primary hepatic or metastatic monophasic SS could also overlap with LMS but is typically positive for EMA and unlikely to express h-caldesmon.
Sarcomatoid hepatocellular carcinoma (ie, very poorly differentiated) (HCC) is rare but could mimic a primary hepatic sarcoma in extreme cases. The degree of moderate (rather than severe) cytologic atypia in the presented case is unlike sarcomatoid HCC, which usually has very atypical cells. Also, even in the most undifferentiated cases, HCC rarely completely loses CK18 positivity, and while divergent expression of muscle markers has been reported, sarcomatoid HCC would be unlikely to strongly express 3 such markers.
Undifferentiated embryonal sarcoma is a primary liver sarcoma that occurs almost exclusively in children typically aged 6-10 years. It is comprised of undifferentiated malignant mesenchymal cells that could be oval, spindled, or anaplastic. Cytoplasmic PAS-positive, diastase-resistant globules are present, while extramedullary hematopoiesis could be seen within the tumor. Although this lesion could occasionally express muscle markers, it is typically CD34 negative and, unlike LMS, is characterized by positive alpha-1-antitrypsin and alpha-1-antichymotrypsin as well as a dot-like pattern with keratins. The absence of many of these features, as well as the age of this patient, argues against embryonal sarcoma.
Supplementary Questions
- Which of the following is correct regarding primary hepatic leiomyosarcoma (hLMS)?
- Any expression of S100 essentially rules out LMS.
- It can arise from the ligamentum teres.
- It is a common hepatic sarcoma in children.
- Its radiologic features are indistinguishable from hepatocellular carcinoma.
- Positive ERG-1 is helpful in confirming LMS.
- Which staining pattern is most consistent with undifferentiated embryonal sarcoma?
- Negative alpha-1 antitrypsin but PASD-positive cytoplasmic globules
- Negative keratin in oval, spindled, and/or anaplastic tumor cells
- Positive CD34, keratin, and alpha-1 antitrypsin
- Positive keratin and PAS positive but PASD negative cytoplasmic globules
- Positive keratin with dot-like pattern and alpha-1 antitrypsin
- Which of the following is the most likely diagnosis for an epithelioid liver tumor expressing DOG-1 and CD34 but negative for ERG-1 and keratin?
- Epithelioid angiosarcoma
- Epithelioid leiomyosarcoma
- Gastrointestinal stromal tumor
- Monophasic synovial sarcoma
- Undifferentiated embryonal sarcoma
References
- Cheng X, Chen D, Chen W, Sheng Q. Primary gastrointestinal stromal tumor of the liver: a case report and review of the literature. Oncol Lett. 2016;12(4):2772-2776.
- Hu X, Forster J, Damjanov I. Primary malignant gastrointestinal stromal tumor of the liver. Arch Pathol Lab Med. 2003;127(12):1606-1608.
- Huang J, Liu Q, Lu JP, Wang F, Wang L, Jin AG. Primary intraluminal leiomyosarcoma of the inferior vena cava: value of MRI with contrast-enhanced MR venography in diagnosis and treatment. Abdom Imaging. 2011;36(3):337-341.
- Jakob M, Schneider M, Hoeller I, Laffer U, Kaderli R. Malignant solitary fibrous tumor involving the liver. World J Gastroenterol. 2013;19(21):3354–3357.
- Lee HJ, Lee JL, Choi WH. A case of primary myxoid leiomyosarcoma of the liver. Korean J Intern Med. 2002;17(4):278-282.
- Matthaei H, Krieg A, Schmelzle M, et al. Long-term survival after surgery for primary hepatic sarcoma in adults. Arch Surg. 2009;144(4):339-344.
- Putra J, Ornvold K. Undifferentiated embryonal sarcoma of the liver: a concise review. Arch Pathol Lab Med. 2015;139(2):269-273.
- Qiu LL, Yu RS, Chen Y, Zhang Q. Sarcomas of abdominal organs: computed tomography and magnetic resonance imaging findings. Semin Ultrasound CT MR. 2011;32(5):405-421.
- Sardaro A, Bardoscia L, Petruzzelli MF, Portaluri M. Epithelioid hemangioendothelioma: an overview and update on a rare vascular tumor. Oncol Rev. 2014;8(2):259.
Author
Oyedele A. Adeyi, MBBS, FCAP
Surgical Pathology Committee
University Health Network / University of Toronto
Toronto, ON, Canada
Answer Key
- It can arise from the ligamentum teres. (b)
- Positive keratin with dot-like pattern and alpha-1 antitrypsin (e)
- Gastrointestinal stromal tumor (c)