Clinical Summary
A 47-year-old man who recently immigrated to the United States from China presents with abdominal fullness, jaundice, and fatigue. Physical exam reveals multiple spider angiomata on the surface of his abdomen and large volume ascites. Liver function tests show mildly elevated alanine aminotransferase (ALT) and aspartate aminotransferase (AST), but normal alkaline phosphatase (AP). Serologic studies are positive for HBsAg (hepatitis B surface antigen) and hepatitis B core antigen (HBcAg). The decision is made to proceed with liver transplantation, and his liver explant specimen is sent for pathologic evaluation. The liver weighs 1828 grams and displays a firm, nodular, dark green surface.
Master List of Diagnoses
- Alpha-1-antitrypsin deficiency
- Autoimmune hepatitis
- Chronic viral hepatitis B
- Chronic viral hepatitis C
- Primary biliary cholangitis
- Primary sclerosing cholangitis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 25, and is chronic viral hepatitis B in the liver.
Criteria for Diagnosis and Comments
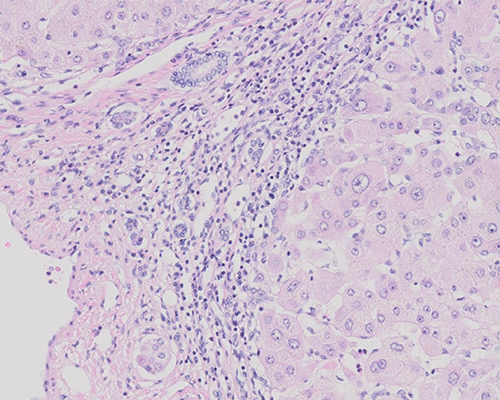
Sections of the explanted liver show distinctive features of chronic hepatitis B virus (HBV) with cirrhosis. The liver parenchyma shows varying degrees of predominantly lymphocytic portal inflammation with moderate interface activity and scattered lobular inflammation. There is diffuse disruption of the hepatic architecture and bridging fibrous septae connecting adjacent portal tracts with Zones 3 and 1 (complete bridging, frank cirrhosis) to one another and to central veins. Round nodules of regenerating hepatocytes are found between the areas of septal fibrosis. Cytologically, hepatocytes demonstrate characteristic “ground-glass” eosinophilic cytoplasm, reflecting the accumulation of hepatitis B surface antigen (HBsAg) within smooth endoplasmic reticulum.
These inclusions are seen on routine H&E staining and signify active viral replication. Special stains, though rarely used, can confirm the nature of these inclusions; these can include Shitaka’s orcein, Victoria blue and aldehyde fuchsin. Immunohistochemical stains for HBsAg (hepatitis B surface antigen) and hepatitis B core antigen (HBcAg) are also available to highlight the viral inclusions. Although “ground-glass” cytoplasm can be helpful in establishing a diagnosis of hepatitis B, this change can also occur in the setting of drug-induced endoplasmic reticulum hypertrophy, cyanamide toxicity, and various storage disorders. Serologic studies for HBV antibodies and HBV DNA are more specific and serve as the primary method for diagnosis and monitoring of patients with hepatitis B. Overall, this constellation of findings best indicate chronic hepatitis B with end-stage liver fibrosis (cirrhosis).
More than 240 million individuals are chronically infected with the hepatitis B virus, an enveloped, double-stranded DNA virus with 8 major genotypes, A-H. There is a higher prevalence in immigrants from sub-Saharan and south Asian countries, and also in those who inject drugs, incarcerated persons, and men who have sex with men. Genotype A is most common in North America and Africa, while types B and C are found primarily in East Asia; type C is also found in southern Europe and India. Type C is associated with more advanced liver fibrosis and increased risk of hepatocellular carcinoma (HCC).
Once infected, the virus forms a highly stabilized double-stranded circular DNA structure within the nucleus of hepatocytes. Viral DNA also integrates into host DNA. Chronic infection results from failure to clear the acute infection and develops in 5%-10% of those acutely infected. Chronic infection is defined by serologic detection of HBsAg on two occasions at least six months apart. Most patients are asymptomatic and detected incidentally after presenting to a health care professional for unrelated reasons. Infants are the most susceptible to chronic infection (90% of infants versus 5%-10% of adults). Chronic infection progresses to cirrhosis in 40% of patients, and 30% of patients with cirrhosis have been reported to develop HCC during a 10-year follow-up interval. Chronic HBV infection accounts for at least 50% of all HCC. HBV can lead to development of HCC even in the absence of cirrhosis (10% of chronically infected patients).
Patients can cycle or alternate through many phases of hepatitis B infection during their lifespan. As the inflammation progresses, it can connect portal tracts with one another as well as to portal veins, resulting in hepatocyte necrosis and deposition of scar tissue. Left untreated, periportal fibrous strands may evolve to bridging fibrosis and ultimately cirrhosis, as is seen in the current case. Despite advancements in biochemical blood tests, evaluation of liver biopsy specimens remains the gold standard for determination of the degree of inflammation and fibrosis.
Although all cirrhotic livers are at increased risk for development of HCC, patients with chronic hepatitis B carry additional risk, independent of the degree of liver injury/fibrosis. This risk is a result of direct viral integration into the host genome, leading to direct oncogenic effects. The overall lifetime risk of developing HCC in patients with chronic HBV is up to 40%. Studies have suggested that HBV-related HCCs may be more aggressive and have a worse prognosis than hepatitis C virus (HCV)-related HCCs. Thus, the role of liver biopsy in these patients also serves to screen for precursor lesions (cirrhosis, liver cell dysplasia) and to identify nodules of well-differentiated HCC. Liver cell dysplasia includes “large liver cell change” (LLCC) and “small liver cell change” (SLCC), which can be seen in various chronic liver diseases. In the current specimen, there are focal areas of LLCC, identified by foci of hepatocytes with cellular enlargement, nuclear pleomorphism with hyperchromasia, and multinucleation. Alternatively, SLCC appears as small cells with a uniform appearance, high nuclear-to-cytoplasmic ratio, and indistinct cytoplasmic borders. Studies have confirmed that SLCC is a true precursor lesion to HCC, while the nature of LLCC remains controversial. Studies regarding the nature of LLCC, as it pertains specifically to HBV-related liver cirrhosis, have shown that in this particular setting, LLCC is more consistent with dysplasia than with reactive hepatocytes.
A chronic hepatitis pattern of injury is not specific for HBV and is also seen in cases of chronic hepatitis C, alcoholic or nonalcoholic steatohepatitis, autoimmune hepatitis, drug-induced liver injury, autoimmune disorders of the biliary tract and various congenital disorders. Specific histologic features may help differentiate these etiologies from chronic hepatitis B.
In cases of chronic viral hepatitis C, the liver typically exhibits prominent periportal lymphoid aggregates macrovesicular steatosis (in genotype 3 HCV) and bile duct damage. The nuclear viral cytopathic effect seen in chronic hepatitis B is not seen in chronic hepatitis C. Liver function studies may be surprisingly normal despite significant periportal inflammation. The fibrosing cholestatic variant of hepatitis C, a particularly devastating and fatal variant, occurs in HCV-infected immunocompromised patients, including a subset of patients who undergo liver transplantation for HCV. These patients have a clinical picture of marked jaundice, cholestatic liver dysfunction and high viral titers. Microscopically, marked hepatocyte swelling, cholestasis, and increased periportal peritrabecular fibrosis are seen, with only mild inflammation. This variant causes fulminant liver failure and rapid graft loss.
Autoimmune hepatitis (AIH) is composed of two variants: AIH-1, which is demonstrates anti-nuclear and/or anti-smooth muscle antibodies (ANA and/or ASMA), and AIH-2, which demonstrates anti-liver kidney microsomal antibody type 1 or 3 (anti-LKM1 or anti-LKM3), and/or anti-liver cytosol antibody type 1 (anti-LC1). Histologically, AIH may be heterogeneous according to the grade and stage of disease but tends to have a prominent lymphoplasmacytic infiltrate and more significant interface and lobular activity as compared with viral hepatitis. Indeed, interface hepatitis is a hallmark of active AIH. While intraepithelial lymphocytes may be seen in bile duct epithelium, bile duct damage is typically not seen in AIH. Hepatocyte rosetting and emperipolesis of lymphocytes may also be seen. Patients are treated with steroids.
In contrast to non-biliary cirrhosis, cases of primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC) will exhibit irregular, jigsaw-puzzle shaped parenchymal nodules and prominent cholestasis. Florid bile duct lesions with granulomatous inflammation further suggest a diagnosis of PBC, while “onion-skin” fibrosis around bile ducts will often times be seen in cases of PSC. Anti-mitochondrial antibodies (AMA) often confirm a diagnosis of PBC, while magnetic resonance cholangiopancreatography would show a “beads on a string” appearance to the biliary tree in PSC patients.
Alpha-1 antitrypsin deficiency may also induce cirrhosis of the liver and demonstrate cytoplasmic inclusions. However, in this disease, the inclusions are small, brightly eosinophilic and only seen in periportal hepatocytes. Staining with PAS-D will highlight the inclusions. Alpha-1-antitrypsin deficiency is an autosomal recessive disorder requiring two mutations of the SERPINA1 gene on chromosome 14 resulting in the PiZZ genotype. 80%-90% of PiZZ individuals may develop chronic liver disease in their 30s-40s, which is ultimately responsible for 10% of deaths due to alpha-1-antitrypsin deficiency. Microscopically, the liver shows intracellular globules of alpha-1-antitrypsin protein, best seen on PAS/D special stain, but also appreciable as eosinophilic globules on H&E stain, with or without frank cirrhosis. There is also a confirmatory immunostain available. Eosinophilic globules are not pathognomonic for the PiZZ state as they may also be seen in the PiMZ genotype. In addition to the peculiar globules, the liver shows variable portal lymphocytic inflammation and mild fat accumulation with mixed micro- and macronodular cirrhosis in a subset of patients. Hepatocyte necrosis is not a prominent feature.
Supplementary Questions
- Which of the following regarding hepatitis C is true?
- Both hepatitis B and hepatitis C can show large droplet steatosis.
- Hepatitis B also shows lymphoplasmacytic portal infiltrates similar to hepatitis C.
- Liver function may be normal despite significant inflammation.
- The fibrosing cholestatic variant of hepatitis C is a frequent finding in grafted livers and confers little clinical significance.
- The fibrosing cholestatic variant of hepatitis C shows moderate to severe portal inflammation.
- Which of the following statements is true?
- Antimitochondrial antibodies are found in cases of primary biliary cholangitis.
- Autoantibodies in autoimmune hepatitis include ANA, AMA, ASMA, anti-LKM1, anti-LKM3, and anti-LC4.
- The inclusions in alpha-1-antitrypsin deficiency are PAS/D sensitive.
- The inclusions in alpha-1-antitrypsin deficiency are pathognomonic to the PiZZ genotype.
- Von Kossa special stain can help identify the intranuclear inclusions in hepatitis B infected livers.
- Which of the following statements regarding hepatitis B is true?
- Chronic HBV accounts for over 80% of all HCC worldwide.
- Hepatitis B Type C is most prevalent in Southeast Asia and is associated with an increased risk of hepatocellular carcinoma.
- Infants are less susceptible to chronic hepatitis B infection than adults.
- Spontaneous clearance of HBV infections can occur in the absence of treatment.
- The intranuclear “ground glass” inclusions are pathognomonic for hepatitis B infection.
References
- Batts KP, Ludwig J. Chronic hepatitis. An update on terminology and reporting. Am J Surg Path. 1995;19(12):1409-1417.
- Chang O, Yano Y,Masuzawa A, Fukushima N, Teramura K, and Hayashi Y. The cytological characteristics of small cell change of dysplasia in small hepatic nodules. Oncol Rep. 2010;23(5):1229-1232.
- Hori T, Onishi Y, Kamei H, et al. Fibrosing Cholestatic hepatitis C in post-transplant adult recipients of liver transplantation. Ann Gastroenterol. 2016;29(4):454-459.
- Kim H, Oh BK, Roncalli M, et al. Large liver cell change in hepatitis B virus–related liver cirrhosis. Hepatology. 2009;50(3):752-762.
- Lefkowitch JH, Schiff ER, Davis GL, et al. Pathological diagnosis of chronic hepatitis C: a multicenter comparative study with chronic hepatitis B. Gastroenterology 1993;104(2):595-603.
- Mani H, and Kleiner DE. Liver biopsy findings in chronic hepatitis B. Hepatology. 2009;49(5 Suppl):S61-71.
- Odze RD, and Goldblum JR. Surgical pathology of the GI tract, liver, biliary tract, and pancreas. Saunders, Elsevier Health Sciences, 2nd edition, Philadelphia, PA, 2009.
- Park YN, and Roncalli M. Large liver cell dysplasia: a controversial entity. J Hepatol. 2006;45(5):734-743.
- Tang LSY, Covert E, Wilson E, and Kottilil S. Chronic Hepatitis B Infection: A Review. JAMA. 2018;319(17):1802-1813.
Author
Yang Zhang, MD
Fellow, Gastrointestinal, Liver, and Pancreas Pathology
The Johns Hopkins Hospital
Baltimore, MD
Sabrina C. Sopha, MD, FCAP
Associate Pathologist
University of Maryland Baltimore Washington Medical Center
Glen Burnie, MD
Answer Key
- Liver function may be normal despite significant inflammation. (c)
- Antimitochondrial antibodies are found in cases of primary biliary cholangitis. (a)
- Spontaneous clearance of HBV infections can occur in the absence of treatment. (d)