- Home
- Member Resources
- Pathology Case Challenge
- Lymph Node, Axilla
Clinical Summary
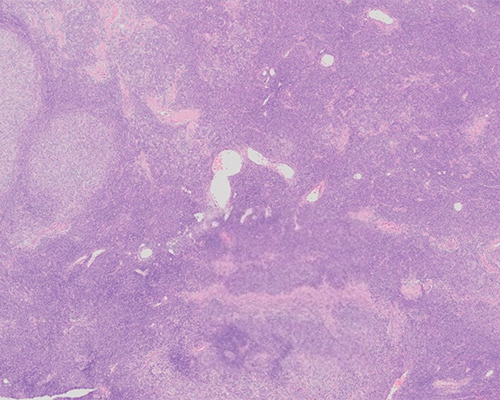
A 61-year-old woman presents with an axillary mass. There are no other systemic symptoms or lymphadenopathy by imaging studies and no other significant past history. An excisional biopsy of the 4 cm mass is performed, and the lymph node tissue is presented for review. Flow cytometry is performed and shows a clonal kappa light chain restricted population of B cells with co-expression of CD10 and lacking CD5. Immunostains reveal that the nodular areas are CD20 positive with co-expression of CD10 and BCL2. CD21 is also positive in these areas, highlighting the dendritic meshwork. The non-nodular areas represent approximately 40% of the nodal surface and lack any CD21-stained meshwork; B cells seen in these areas co-express CD10 and BCL2.
Master List of Diagnoses
- Classic Hodgkin lymphoma, nodular sclerosis type
- Diffuse large B-cell lymphoma
- Classic follicular lymphoma
- Mantle cell lymphoma
- Nodal marginal zone lymphoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 20, and is Follicular lymphoma, follicular and diffuse, low grade (grade 1-2) in an axillary lymph node.
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
Histological features reveal effacement of lymph nodal architecture with a nodular and diffuse proliferation composed of a mixture of small cleaved centrocytes and intermingled large centroblasts. Sclerotic bands are also seen both within and surrounding the nodular areas. Based on the flow cytometry, H&E slide morphology and immunostains, the diagnosis is classic follicular lymphoma (FL) with a mixed follicular and diffuse pattern.
FL is a very common lymphoma in the Western Hemisphere, comprising about 20% of all lymphomas. Environmental exposure to pesticides and herbicides has been associated with an increased risk of this non-Hodgkin lymphoma. The current World Health Organization (WHO 5e) identifies a few variants of follicular lymphoma and distinguishes certain patterns of this disease. A distinct type of follicular lymphoma seen in the pediatric age group is designated as pediatric-type FL. This is an uncommon nodal FL that is seen mostly in the head and neck and presents with stage 1 disease. Even though cytologically the pediatric type FL appears to be of high grade (increased centroblasts), the prognosis is excellent. Duodenal-type FL is another distinct variety, where the lymphoid proliferation is seen in the small intestine (commonly duodenum). Extranodal FL tend to have a higher grade and frequently lacks BCL2 protein and a BCL2 translocation, such as t(14;18). FL with an expanded marginal zone, or morphologically appearing similar to progressive transformation of germinal centers, has been termed the “floral variant” of FL. Similarly, FL where most of the centrocytes resemble signet ring cells (signet-ring variant) has also been reported.
Most cases of FL have a predominantly follicular pattern, with closely packed follicles that efface the nodal architecture. The follicles lack tingible body macrophages and polarization. The follicles are composed of small cleaved centrocytes and scattered large centroblasts. The proportion of centroblasts is enumerated based on the Mann–Berard system of grading. Grading in the new WHO 5e is not necessary but remains optional. Grade 1 has 0 - 5 centroblasts/high-power field (HPF), grade 2 has 6 - 15 centroblasts/HPF, and grade 3 has greater than 15 centroblasts/HPF. Grade 3 FL is further divided into grades 3A and 3B: If the centrocytes are mixed with centroblasts, then it is graded as 3A, whereas centroblasts in diffuse sheets constitutes grade 3B FL. WHO5e designates FL grade 1, 2, and 3A as classic follicular lymphoma due to lack of reproducibility in grading and the lack of statistical significance between clinical outcomes. Grade 3B FL, renamed follicular large B cell lymphoma in WHO5e, clinically behaves similar to diffuse large B-cell lymphoma.
Spread of FL beyond the lymph node capsule or to extra-nodal locations, specifically the retro-peritoneum and mesentery, tends to cause sclerosis (so-called sclerosing variant of FL). In excisional specimens such as this case, the WHO5e no longer recommends that the relative proportions of follicular and diffuse areas be noted in the final pathology report. Diffuse areas of FL should not be confused with reactive lymph node paracortex, which are T cell-rich and should lack lymphoma cells as demonstrated by immunostains. These diffuse areas should also lack a CD21/CD23-positive follicular dendritic meshwork. Of note, the diffuse areas should be composed of mostly small centrocytes. Diffuse sheets of centroblasts/large cells in areas devoid of dendritic reticulum cell meshwork fulfill criteria for diffuse large B-cell lymphoma transformation and should be notated as such.
Classic Hodgkin lymphoma (CHL) is not a consideration, since the nodal proliferation shows a predominantly small, cleaved morphology and lacks classic Reed–Sternberg cells. Additionally, flow cytometry shows a clonal B-cell population that is CD10-positive.
Diffuse large B-cell lymphoma (DLBCL) is another common lymphoma in the Western Hemisphere. It is a higher-grade lymphoma and frequently arises de novo but can also be seen as transformation from any type of low-grade lymphoma. Diffuse sheets of large B cells are the most common morphologic finding in DLBCL. Admixture of predominantly small cells (centrocytes) or the presence of follicles will preclude this diagnosis.
Mantle cell lymphoma is an intermediate-grade lymphoma of mature B cells that aberrantly co-express CD5. Cyclin D1 is the driver of this lymphoma, and the neoplastic B cells show stainable cyclin D1. Recently, a subset of cyclin D1-negative mantle cell lymphomas that expresses SOX11 has been recognized.
Nodal marginal zone lymphoma is another type of low-grade non-Hodgkin lymphoma, with predominantly marginal zone expansion and clonal proliferation of marginal zone B cells. Unlike this case, CD10 is not expressed aberrantly in marginal zone lymphoma. In a subset of cases, aberrant CD43 co-expression may be seen.
Supplementary Questions
- Which of the following is true regarding diffuse areas in follicular lymphoma (FL)?
- CD25 is the marker of choice when evaluating dendritic reticular meshwork within diffuse areas.
- Diffuse areas in FL almost always represent paracortical zones of T cells.
- Diffuse areas in FL are the equivalent of a higher grade (grade 3).
- Diffuse areas of small neoplastic centrocytes exist in FL and should be devoid of CD21-positive dendritic cell meshwork.
- Diffuse areas should not exist in FL; if they are seen, then the diagnosis is diffuse large B-cell lymphoma.
- A mesenteric biopsy in a 68-year-old man shows dense sclerosis with many follicles composed of CD10-positive, BCL2-positive small B cells, which are kappa light chain restricted by flow cytometry. Which of the following may be a diagnostic consideration?
- Diffuse large B-cell lymphoma
- Florid reactive follicular hyperplasia
- Nodular sclerosis classic Hodgkin lymphoma
- Pediatric-type FL
- Sclerosing variant of FL
- Excisional biopsy of a lymph node reveals FL with back-to-back follicles in 80% of the specimen, with predominantly centrocytes within these follicles. In the remainder of the section, no demonstrable CD21/CD23-positive dendritic reticulum cell meshwork is seen, and there are sheets of centroblasts without any admixed centrocytes. How is this lymphoma best classified?
- Follicular large B cell lymphoma and diffuse large B-cell lymphoma
- Diffuse large B cell lymphoma
- Follicular large B cell lymphoma
- Classic FL
- FL, unclassifiable
References
- Choi SM, Betz BL, Perry AM. Follicular lymphoma Diagnostic Caveats and Updates. Arch Pathol Lab Med. 2018;142(11):1330-1340.
- Younes SF, Beck AF, Lossos IS, Levy R, Warnke RA, Natkunam Y. Immunoarchitectural patterns in follicular lymphoma: efficacy of HGAL and LMO2 in the detection of the interfollicular and diffuse components. Am J Surg Pathol. 2010;34(9):1266-1276.
- Horn H, Schmelter C, Leich E, et al. Follicular lymphoma grade 3B is a distinct neoplasm according to cytogenetic and immunohistochemical profiles. Haematologica. 2011;96(9):1327-1334.
- WHO classification of tumours Editoral Board. Hematolymphoid tumors. Lyon (France): International Agency for Research on Cancer, forthcoming. (WHO classification of tumors series, 5ht ed; vol.11). https://publications.iarc.fr
Answer Key
- Diffuse areas of small neoplastic centrocytes exist in FL and should be devoid of CD21-positive dendritic cell meshwork. (d)
- Sclerosing variant of FL (e)
- Follicular large B cell lymphoma and diffuse large B-cell lymphoma (a)