Clinical Summary
A 51-year-old woman presents with abdominal discomfort and ascites. Imaging studies reveal bilateral ovarian masses, and the patient subsequently undergoes total hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and bilateral pelvic and para-aortic lymph node dissection. Intraoperatively, miliary omental nodules are also noted. Gross examination reveals multiple yellow-tan nodules, ranging from 0.2-1.5 cm, studding the surfaces of both ovaries and the omentum. Immunohistochemistry shows the tumor cells are positive for calretinin, WT1, and PAX8, while negative for Ber-EP4 and MOC-31.
Master List of Diagnoses
- Adenomatoid tumor
- Low-grade serous carcinoma
- Malignant mesothelioma
- Serous borderline tumor
- Well-differentiated papillary mesothelioma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 18, and is well-differentiated papillary mesothelioma of the ovary.
Criteria for Diagnosis and Comments
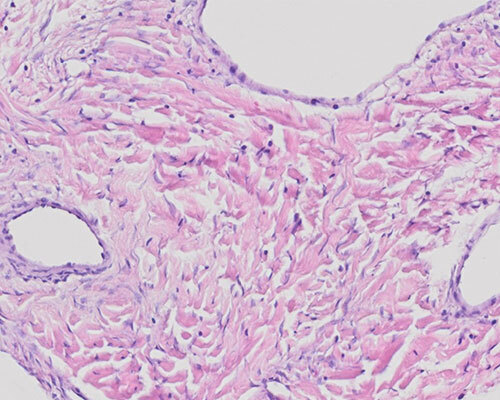
The slides show a papillary proliferation with occasionally hyalinized or foamy macrophage-containing fibrovascular cores lined by a single layer of cuboidal or attenuated cells. Nuclear atypia is minimal and only rare mitotic figures are identified. Some slides show focal psammomatous calcifications, while others show rare tubular architecture. Destructive infiltration of the underlying stroma is not identified. The overall morphologic features and immunohistochemical findings are consistent with a diagnosis of well-differentiated papillary mesothelioma (WDPM).
WDPM is a rare tumor predominantly affecting reproductive-age women, although cases occurring in postmenopausal patients have been reported. The lesions are usually discovered incidentally; however, less commonly—as in this case—ascites and/or abdominal pain may be present. Solitary or multiple small (less than 2 cm), firm, nodular lesions are identified grossly. In contrast with pleural lesions, WDPM of the peritoneum has only rarely been reported in association with a history of asbestos exposure. Excision of WDPM is considered curative; very few instances of recurrence have been reported.
While peritoneal malignant mesotheliomas (PMM) may show focal well-differentiated papillary areas, care should be taken not to overcall WDPM, particularly since the prognosis for WDPM is much more favorable than that of PMM. Thorough sampling should be performed to aid in accurate characterization. Identification of other growth patterns may help distinguish between the 2 lesions; solid architecture or biphasic, sarcomatoid, or deciduoid features are not typical of WDPM. Although nuclear atypia may be mild in both lesions, the presence of moderate or severe atypia, extensive pseudostratification, or more than rare mitotic figures favors PMM over WDPM. Grossly, PMM is typically characterized by more diffuse peritoneal involvement by larger lesions, often described as plaques, than in WDPM. While stromal invasion of underlying peritoneal surfaces is usually present in PMM, this is not a feature of WDPM.
Adenomatoid tumor shares many characteristics with WDPM, as it is also an uncommon, often incidental, benign neoplasm of mesothelial origin, not associated with asbestos exposure. These tumors are usually small, solid, and more likely to involve the fallopian tube, ovary, and myometrium, although omental and mesenteric lesions are not uncommon. While the microscopic appearance is variable, and papillae may be encountered, the cells of adenomatoid tumors most frequently form anastomosing gland-like spaces with varying degrees of cystic dilatation.
PMM, adenomatoid tumor, and WDPM are all lesions of mesothelial origin, and they have similar immunophenotypic profile—positive staining for CK5/6, calretinin, WT1, and HBME-1. Therefore, immunohistochemistry is of limited use in distinguishing among these lesions. Interestingly, however, while PAX8 is negative in PMM and a reliable distinguisher between malignant mesothelioma and ovarian serous neoplasms, several recent studies have reported PAX8 expression in WDPM.
Serous borderline tumors (SBT), also known as atypical proliferative serous tumors, often display florid papillae involving the surface of the ovaries and other peritoneal surfaces, similar to WDPM. However, SBT differ in that they usually also involve the ovarian parenchyma. In addition, the papillae have a characteristically hierarchical branching pattern and are lined by taller columnar cells with rare cuboidal cells, contrasting with the predominantly flattened to cuboidal cells of WDPM.
Low-grade serous carcinoma (LGSC) frequently presents as this patient did, with ascites and bilateral ovarian lesions. However, LGSC is an invasive tumor, with haphazard stromal infiltration by single cells, irregular small nests, and micropapillae with an inconspicuous or absent stromal core. Macropapillae may also be present, although less common. Invasive foci of both micro- and macropapillae are typically surrounded by a clear unlined space. LGSC displays mild to moderate nuclear atypia and increased mitotic activity (although usually fewer than 2-3 per 10 high power fields) compared to WDPM.
Psammoma bodies are common in SBT and LGSC, and both these tumors stain with cytokeratin, EMA, WT1, and PAX8, with wild-type p53 expression. While WDPM are also WT1 positive with reported PAX8 expression and may occasionally display psammoma bodies, they are typically negative for markers of epithelial differentiation including Ber-EP4, MOC-31, and B72.3, unlike low-grade serous neoplasms. A panel of immunostains, including both epithelial and mesothelial cell markers, may aid in characterization.
Supplementary Questions
- Which of the following is true of well-differentiated papillary mesothelioma (WDPM)?
- Standard management for WDPM includes adjuvant chemotherapy.
- WDPM is typically associated with a history of asbestos exposure.
- WDPM is typically MOC31-positive and CK5/6-negative.
- WDPM is usually an incidental finding, predominately affecting women.
- WDPMs tend to form large peritoneal plaques.
- The presence of which of the following favors a diagnosis of serous borderline tumor over WDPM?
- Ber-EP4 expression
- Cuboidal cells
- PAX8 expression
- Psammoma bodies
- WT1 expression
- The presence of which of the following favors a diagnosis of peritoneal malignant mesothelioma over WDPM?
- HBME-1 expression
- Minimal cytologic atypia
- Papillae with hierarchical branching
- Small solitary lesion
- Stromal infiltration of underlying tissues
References
- Baker PM, Clement PB, Young RH. Selected topics in peritoneal pathology. Int J Gynecol Pathol. 2014;33(4):393-401.
- Chen X, Sheng W, Wang J. Well-differentiated papillary mesothelioma: a clinicopathological and immunohistochemical study of 18 cases. Histopathology. 2013;62(5):805-813.
- Husain AN, Colby TV, Ordóñez NG, et al. Guidelines for pathologic diagnosis of malignant mesothelioma 2017 update of the consensus statement from the International Mesothelioma Interest Group. Arch Pathol Lab Med. 2018;142:89-108.
- Kurman RJ, Carcangiu ML, Herrington CS, Young RH, eds. WHO Classification of Tumours of Female Reproductive Organs. 4th ed. Lyon, France: IARC; 2014:18-21,90-91.
- Laury AR, Hornick JL, Perets R, et al. PAX8 reliably distinguishes ovarian serous tumors from malignant mesothelioma. Am J Surg Pathol. 2010;34(5):627-635.
- Malpica A, Sant’Ambrogio S, Deavers MT, Silva EG. Well-differentiated papillary mesothelioma of the female peritoneum: a clinicopathologic study of 26 cases. Am J Surg Pathol. 2012;36:117-127.
- Xing D, Banet N, Sharma R, Vang R, Ronnett BM, Illei PB. Aberrant Pax-8 expression in well-differentiated papillary mesothelioma and malignant mesothelioma of the peritoneum: a clinicopathologic study. Hum Pathol. 2018;72:160-166.
Author
Rochelle A. Simon, MD, FCAP
Surgical Pathology Committee
The George Washington University
Washington, DC
Answer Key
- WDPM is usually an incidental finding, predominately affecting women. (d)
- Ber-EP4 expression (a)
- Stromal infiltration of underlying tissues (e)