Clinical Summary
A 45-year-old nulliparous woman presents with a history of mild abdominal pain of three months’ duration. Ultrasound reveals a 10 cm well-defined lobulated right adnexal mass. Total abdominal hysterectomy with bilateral salpingo-oophorectomy and partial omentectomy is performed. Grossly, the tumor measures 9.5 cm in maximum dimension, with a multilobulated glistening white nodular surface. The cut surface shows well-circumscribed whitish nodules surrounded by fibrous tissue.
Master List of Diagnoses
- Benign Brenner tumor
- Borderline Brenner tumor
- Carcinoid tumor
- Granulosa cell tumor
- Malignant Brenner tumor
- Metastatic low-grade urothelial carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 24, and is a benign Brenner tumor in the ovary.
Criteria for Diagnosis and Comments
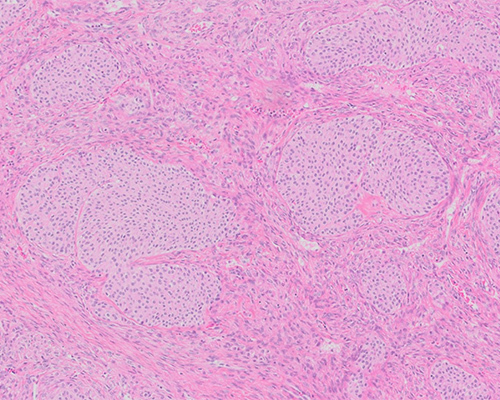
Histologic examination shows well-circumscribed solid epithelial cell nests surrounded by abundant fibrous stroma. The epithelial cells are ovoid to polygonal and have pale cytoplasm and oval nuclei. Some of the nuclei have central longitudinal grooves (“coffee-bean” appearance). These histologic features are consistent with a diagnosis of benign Brenner tumor of the ovary.
Most primary tumors of the ovary are divided into one of three major categories: surface epithelial-stromal tumors, sex cord-stromal tumors, and germ cell tumors. Brenner tumors, a type of surface epithelial-stromal tumor of the ovary, were first described by Fritz Brenner in 1907. They are rare neoplasms accounting for about 1% to 2% of all ovarian tumors. The World Health Organization (WHO) classifies Brenner tumors (BT) into three categories: benign, borderline (atypical proliferative transitional cell tumor) and malignant. Borderline BT and malignant BT account for only 0.5% of ovarian transitional cell tumors (Brenner tumors).
Most BT occur between the ages of 30 and 70 years. More than half of borderline BT, and more than 65% of malignant BT, are diagnosed in women 50 to 70 years of age. Patients may present with vaginal bleeding, a slow-growing palpable mass, and pelvic/abdominal pain. Sometimes BT are associated with estrogenic or, less often, androgenic symptoms as a result of steroid hormone secretion by their stromal component. BT may be associated with other primary ovarian tumors, including mucinous neoplasms, mature cystic teratoma, and struma ovarii.
Benign BT are typically small and often an incidental finding; half are less than 2 cm, and about 10% are bilateral. Grossly, benign BT are solid, nodular, lobulated, well-circumscribed masses with hard or fibromatous, gray, white, or slightly yellow cut surfaces. Occasionally, the tissue becomes gritty because of calcified deposits. The tumors may show small (or rarely large) cysts, and rare cases are multicystic. Borderline BT are almost always unilateral and typically have solid and cystic components, with the former resembling benign BT and the latter usually containing papillae or polyps. Malignant BT typically have both solid and cystic areas, with the latter containing papillary or polypoid masses or mural nodules. About 10% are bilateral.
Microscopically, benign BT show transitional epithelium-type (urothelial-like) cells arranged in well-defined, solid or partially cystic nests, as well as trabeculae. The cells have pale cytoplasm and oval nuclei that may contain grooves. No cytologic atypia is present, and mitotic figures are rare. The epithelial cells are admixed with dense, fibrotic stroma that sometimes contains calcifications. The stromal component resembles an ovarian fibroma and occasionally contains luteinized cells. Cysts lined by mucinous or other glandular epithelium and filled with eosinophilic material may be seen. The mucinous component can be distinct enough to qualify for an associated mucinous neoplasm, usually mucinous cystadenoma, in up to 16% of BT.
Borderline BT show atypical urothelial-like cells in poorly defined nests, with focal necrosis and occasional mitoses; no stromal invasion is present. Cystic components are often present, with papillary intraluminal projections.
Malignant BT can resemble urothelial or rarely squamous carcinomas but are defined by their association with either a benign or borderline Brenner component. Malignant BT show pleomorphic, mitotically active cells invading singly and in nests. Stromal invasion with desmoplasia and occasional necrosis must be present for the diagnosis of malignant BT.
Immunohistochemical stains are usually not required for the diagnosis of Brenner tumor. Benign and borderline Brenner tumors show positivity for CK7 and are negative for CK20, similar to other primary ovarian epithelial tumors. They are also positive for urothelial markers, including p63 (diffuse nuclear staining), uroplakin III (luminal staining), thrombomodulin (membranous staining) and GATA3. Of note, uroplakin III is the most specific of these markers for urothelial differentiation. The invasive component of malignant Brenner tumors may have a more variable expression of these markers.
Most BT are candidates for surgical resection. Because of their circumscribed nature, benign and borderline BT are easily located and do not typically affect surrounding tissue. Oophorectomy is curative and will reverse any symptoms related to mass effect or functioning stroma. The majority of malignant BT are also localized to one ovary and have an excellent prognosis. Regional lymph node spread is uncommon. As with other surface epithelial ovarian tumors, stage is the most important predictor; malignant BT with extra-ovarian spread are associated with a poor outcome.
The histogenesis of ovarian Brenner tumors is controversial. Possible origins include ovarian surface epithelium, mesonephric remnants, rete ovarii, teratomas, and Walthard cell nests. The most compelling of these is Walthard cell nests, which are postulated to arise from transitional cell metaplasia of tuboperitoneal junction cells. These nests then implant onto the ovary, where they develop into Brenner tumors.
Although transitional cell carcinoma of the ovary is still included in the WHO classification of tumors of female reproductive organs, most of these likely represent either high-grade serous or poorly differentiated endometrioid carcinomas with transitional-like morphology. Furthermore, the frequent finding of WT1 nuclear expression in transitional-appearing carcinomas supports serous differentiation, and the fallopian tubes should be carefully examined for the presence of serous tubal intraepithelial carcinoma (STIC).
Carcinoid tumor, insular type, may resemble BT due to the presence of solid nests within fibromatous stroma. The nuclei in carcinoid tumors are round and hyperchromatic with stippled chromatin. The cytoplasm is eosinophilic with red or brown argentaffin granules. Immunostains are positive for neuroendocrine markers (synaptophysin and chromogranin).
Granulosa cell tumor, a type of sex cord-stromal tumor, can have an insular pattern simulating that of a benign Brenner tumor or a papillary cystic pattern suggesting a borderline BT. Granulosa cell tumors are composed of small, bland, and cuboidal to polygonal cells with coffee-bean nuclei arranged in various patterns, including microfollicular, macrofollicular, trabecular, solid and insular. The cells are positive for inhibin, calretinin, and steroidogenic factor 1 (SF1); they are negative for CK7 and for urothelial markers.
A patient’s previous history of urothelial carcinoma is the most helpful in making a diagnosis of metastatic low-grade urothelial carcinoma. Widespread disease is uncommon in BT, and the combination of multiple small nodules in bilateral ovaries, disease involving the ovarian surface and lymph-vascular invasion favors a metastatic origin.
Supplementary Questions
- Which primary ovarian neoplasm is most commonly seen in association with benign Brenner tumor?
- Carcinoid tumor
- Fibroma
- Mucinous cystadenoma
- Serous cystadenoma
- Sertoli cell tumor
- Which of the following histologic findings are characteristic of benign Brenner tumor?
- Coffee bean-shaped cells arranged in a microfollicular pattern
- Cysts lined by mucinous glandular epithelium
- Sheets of lipid-rich theca cells admixed with fibrous stroma
- Spindle cells arranged in a storiform pattern with intracellular edema
- Well-defined solid nests of transitional cells within dense fibrous stroma
- Which of the following is the most specific urothelial cell marker?
- CK7
- GATA3
- HMWCK
- Thrombomodulin
- Uroplakin III
References
- Ali RH, Seidman JD, Luk M, Kalloger S, and Gilks CB. Transitional cell carcinoma of the ovary is related to high-grade serous carcinoma and is distinct from malignant Brenner tumor. Int J Gynecol Pathol. 2012;31(6):499-506.
- Esheba GE, Longacre TA, Atkins KA, Higgins JP. Expression of the urothelial differentiation markers GATA3 and placental S100 (S100P) in female genital tract transitional cell proliferations. Am J Surg Pathol. 2009;33:347-353.
- Gilks CB, Carinelli SG, Liu A, et al. Brenner tumours. In: Kurman RJ, Carcangiu ML, Herrington CS, Young RH, eds. WHO Classification of Tumours of Female Reproductive Organs. Lyon: International Agency for Research on Cancer. 2014;35-37.
- Nasioudis D, Sisti G, Holcomb K, Kanninen T, Witkin S. Malignant Brenner tumors of the ovary; a population-based analysis. Gynecol Oncol. 2016;142(1):44-49.
- Seidman JD, Khedmati F. Exploring the histogenesis of ovarian mucinous and transitional cell (Brenner) neoplasms and their relationship with Walthard cell nests. Arch Pathol Lab Med. 2008;1753-1760.
- St Pierre-Robson K, Dunn PJ, Cooper E, et al. Three cases of an unusual pattern of invasion in malignant Brenner tumors. Int J Gynecol Pathol. 2013;32(1):31–34.
- Takeuchi T, Ohishi Y, Imamura H, et al. Ovarian transitional cell carcinoma represents a poorly differentiated form of high-grade serous or endometrioid adenocarcinoma. Am J Surg Pathol. 2013;37:1091-1099.
Author
Archi Patel, MD
Surgical Pathology Committee, Jr Member
East Tennessee State University
Johnson City, TN
Answer Key
- Mucinous cystadenoma (c)
- Well-defined solid nests of transitional cells with dense fibrous stroma (e)
- Uroplakin III (e)