Clinical Summary
A 58-year-old woman with a prior history of pancreatic adenocarcinoma presents with abdominal pain and is found to have a 9 cm cystic left adnexal mass. The patient undergoes a hysterectomy and bilateral salpingo-oophorectomy. Gross examination of the left ovary shows a smooth serosal surface with a surgical defect. Sectioning shows an 8 cm cyst and some smaller cysts with hemorrhagic and fibrinous debris and clot. The right ovary has a 1 cm hemorrhagic cyst, which is benign on histology. The uterus is unremarkable histologically. The ovarian tumor is diffusely and strongly positive for CK7 and CK20. CDX2 shows focal positivity. PAX8 is negative. SMAD4 expression is lost. A background precursor lesion is not identified.
Master List of Diagnoses
- Endometrioid carcinoma of ovary
- Metastatic colonic adenocarcinoma
- Metastatic endocervical adenocarcinoma
- Metastatic pancreatic ductal adenocarcinoma
- Mucinous carcinoma of ovary
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 37, and is metastatic pancreatic ductal adenocarcinoma in the ovary.
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
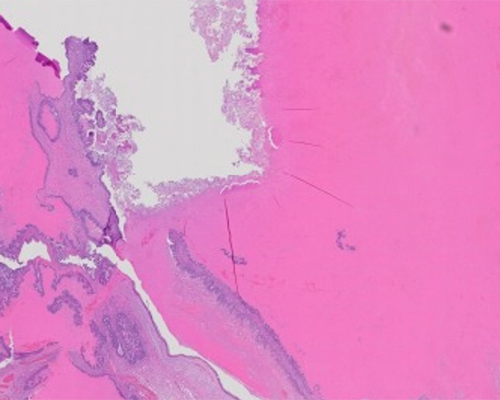
Microscopic sections of the ovary show variably sized cysts with necrotic debris. The cysts show garlanding by pseudostratified glandular epithelium. Some of the epithelium is mucin-depleted, while other areas show overt mucinous differentiation. The mucinous epithelium shows primarily a foveolar (upper gastrointestinal) phenotype, although occasional areas with goblet cells are present on some slides. The epithelium ranges from bland to atypical, with atypical areas showing moderate atypia with only occasional mitotic figures. Endometriosis is not identified. There is no evidence of a co-existent teratoma, Brenner tumor, or carcinoid neoplasm. The immunohistochemical profile (CK7 positive, CK20 positive, CDX2 patchy positive, and SMAD4 loss), especially with the clinical history of prior pancreatic carcinoma, is consistent with metastatic pancreatic ductal adenocarcinoma. Other histologic findings that may aid in the diagnosis of metastatic pancreatic ductal adenocarcinoma (not seen in this case) include a nodular or infiltrative pattern of growth with prominent desmoplasia and abrupt transition from low- to high-grade nuclear atypia in the epithelium. Mitotic activity is often modest and disproportionate to the degree of nuclear atypia. Generous sampling of the tumor may be needed to identify areas with more characteristic findings.
SMAD4 loss is seen in about 58% of pancreatic carcinoma. However, SMAD4 loss may also be seen in as many as 30% of colonic/appendiceal adenocarcinomas, in a small percentage of gastric carcinoma, and even in some endocervical mucinous carcinoma, among others. Therefore, the SMAD4 loss should be interpreted in the context of clinical history and presentation, and comparison with the patient’s prior primary carcinoma.
Metastatic carcinomas to the ovary are usually less than 10 cm in size, bilateral, show solid, and cystic areas with serosal involvement and often have associated intra-abdominal metastases. However, they can be unilateral and large, predominantly cystic, and show a smooth serosal surface and thus mimic primary mucinous ovarian carcinoma (PMOC). Borderline or even benign-looking areas can be present in metastatic mucinous carcinoma to the ovary, further confounding distinction from primary ovarian tumors.
PMOC is typically strongly positive for CK7, with variable expression of CK20 and CDX2. They are usually limited to the ovary at presentation. Extensive extra-ovarian tumor should raise suspicion for a possible metastatic mucinous carcinoma to the ovary. PAX8 and ER positivity are diagnostic of PMOC; however, these immunostains may be negative. PMOC arise in different contexts, and this is reflected in the varied immunohistochemical profiles that these tumors can show. Tumors arising from the gastrointestinal component of a teratoma are likely to express a strong colonic adenocarcinoma immunohistochemical and molecular profile, such as diffuse and strong CDX2, SATB2, and CK20 positivity, and absent or markedly reduced expression of CK7. They often show mutations of RNF43 that are characteristic of gastrointestinal carcinoma. Mucinous carcinomas arising from Brenner tumors, on the other hand, show a somewhat less well-developed gastrointestinal profile and lack both the strong expression of SATB2 and the RNF43 mutations of teratoma-derived ovarian mucinous carcinoma.
Metastatic endocervical adenocarcinoma may arise from either human papillomavirus (HPV)-associated or non-HPV-associated mechanisms. HPV-associated endocervical carcinoma is readily distinguished from metastatic pancreatic adenocarcinoma. In addition to showing the characteristic morphology of “floating mitoses” and basal apoptosis, it is HRHPV and PAX8 positive, with a wild-type p53 expression pattern. (Note: p16 should not be used as a surrogate for HPV-derived carcinoma in this setting, as many carcinomas, including pancreatic carcinoma, show p16 positivity from HPV-independent pathways.)
Metastases from non-HPV endocervical adenocarcinoma, especially the gastric type and minimal deviation adenocarcinoma (GEA/MDA), pose a challenge with respect to distinction from a metastatic pancreatic ductal adenocarcinoma. GEA/MDA is an aggressive adenocarcinoma that has overlapping clinical, histological, and immunohistochemical profile with pancreatic adenocarcinomas. GEA/MDA can show intraabdominal dissemination with metastases to the omentum and ovaries. TP53 mutations with attendant aberrant p53 expression is also common, similar to pancreatic carcinoma, and like pancreatic carcinoma, it is HRHPV negative. The homology between GEA/MDA and pancreatic ductal adenocarcinoma is perhaps not surprising, as both MDA and pancreatic ductal adenocarcinoma are associated with mutations in STK11. Both tumors are therefore also part of the constellation of tumors seen in Peutz–Jeghers syndrome, where there is a germline mutation in STK11. While PAX8 may be negative in GEA/MDA, it may discriminate between a GEA/MDA and a metastatic pancreatic adenocarcinoma when positive. Pancreatic carcinoma is typically negative for PAX8.
Primary endometrioid carcinomas of the ovary commonly arise in a background of endometriosis. They often show squamous or morular metaplasia. They are typically positive for CK7, PAX8, and hormone receptors. CDX2 and SATB2 positivity is restricted to areas with morular metaplasia; the glandular areas are typically negative for these markers.
Metastatic colonic adenocarcinoma characteristically shows “dirty necrosis” with a garlanding pattern of growth (seen in some areas in this case). However, the typical colonic carcinoma shows either prominent diffuse goblet cell differentiation or a mucin-depleted cytology with abundant mitotic figures. Extensive foveolar (upper gastrointestinal) mucinous differentiation is uncommon. CK20, CDX2, and SATB2 positivity is characteristically diffuse and strong. CK7 is typically negative or weakly expressed. Variant immunohistochemical profiles of colonic adenocarcinoma that are CK20/CDX2 negative and CK7 positive are distinctly uncommon and seen primarily in the setting of Lynch syndrome.
Supplementary Questions
- Which of the following is true of metastatic pancreatic ductal adenocarcinoma to the ovary?
- Areas can mimic benign or borderline ovarian tumors.
- Areas commonly show dirty necrosis and a garlanding growth pattern.
- It commonly shows floating mitoses.
- It is commonly unilateral and greater than 10 cm in size.
- Retention of SMAD4 expression rules out pancreatic origin.
- Which of the following is true regarding mucinous carcinoma of the ovary arising from teratoma?
- It commonly coexists with a Brenner tumor.
- It commonly coexists with endometriosis.
- It is diffusely and strongly positive for CK7.
- It is diffusely and strongly positive for p16.
- It is diffusely and strongly positive for SATB2.
- In a patient with prior history of pancreatic ductal adenocarcinoma and new ovarian mass, which of the following immunohistochemical profiles favors a primary ovarian mucinous carcinoma?
- CK7-/CDX2+/SATB2+
- CK7-/CK20+/CDX2+
- CK7-/CK20+/SATB2+
- CK7+/CK20+/PAX8-
- CK7+/CK20+/PAX8+
References
- Carleton C, Hoang L, Sah S, et al. A detailed immunohistochemical analysis of a large series of cervical and vaginal gastric type adenocarcinomas. Am J Surg Pathol. 2016;40(5):636-644.
- Hodgson A, Park KJ. Cervical Adenocarcinomas: A Heterogeneous Group of Tumors With Variable Etiologies and Clinical Outcomes. Arch Pathol Lab Med. 2019;143(1):34-46.
- WHO Classification of Tumours Editorial Board. Female genital tumours [Internet]. IARC Press; 2020. (WHO classification of tumours series, 5th ed.; vol. 4). Available from: https://tumourclassification.iarc.who.int/chapters/34;
- McCluggage WG, Van de Vijver K. SATB2 is Consistently Expressed in Squamous Morules Associated With Endometrioid Proliferative Lesions and in the Stroma of Atypical Polypoid Adenomyoma. Int J Gynecol Pathol. 2018;38(5):397-403.
- Ohtsubo K, Watanabe H, Yamaguchi Y, et al. Abnormalities of tumor suppressor gene p16 in pancreatic carcinoma: immunohistochemical and genetic findings compared with clinicopathological parameters. J Gastroenterol. 2003;38(7):663-671.
- Ritterhouse LL, Wu EY, Kim WG, Dillon DA et al. Loss of SMAD4 protein expression in gastrointestinal and extra-gastrointestinal carcinomas. Histopathology. 2019;75:546-551.
- Simons M, Simmer F, Bulten J, et al. Two types of primary mucinous ovarian tumors can be distinguished based on their origin. Mod Pathol. 2020;33(4):722-733.
Answer Key
- Areas can mimic benign or borderline ovarian tumors. (a)
- It is diffusely and strongly positive for SATB2. (e)
- CK7+/CK20+/PAX8+ (e)