- Home
- Member Resources
- Pathology Case Challenge
- Parotid Gland
Clinical Summary
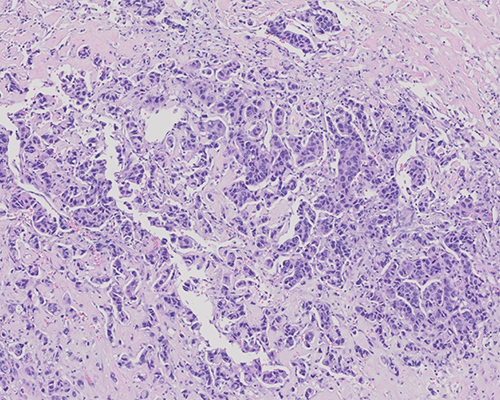
A 70-year-old man presents with a rapidly growing right cheek mass with associated pain, facial nerve palsy, and cervical lymphadenopathy. The right parotid is resected and shows an ill-defined 5 cm firm white mass. The tumor is positive for GCDFP15 and androgen receptor (AR).
Master List of Diagnoses
- Acinic cell carcinoma
- Adenoid cystic carcinoma
- Mucoepidermoid carcinoma
- Salivary duct carcinoma
- Secretory carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 07, and is salivary duct carcinoma in the parotid gland.
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
Sections show a tumor comprised of neoplastic cells with variable amounts of “Roman bridging” architecture present. An invasive solid or micropapillary component predominates in many slides. The tumor cells are polygonal with moderately pleomorphic, hyperchromatic nuclei with coarse chromatin, prominent nucleoli, and ample eosinophilic, granular cytoplasm. A highly desmoplastic stroma is present. Atypical mitoses and comedonecrosis are variably present, as well as perineural invasion on some slides. The tumor is strongly positive for GCDFP15 and androgen receptor (AR). The overall findings are characteristic of salivary duct carcinoma (SDC).
SDC are high-grade adenocarcinomas that can either arise de novo or present as the malignant component of a carcinoma ex pleomorphic adenoma. They have been reported to comprise anywhere from 1% to 10% of all salivary gland malignancies and tend to occur in men, with the peak incidence in the sixth and seventh decades. They most often occur in the parotid and present as a rapidly growing tumor with facial nerve involvement. The prognosis is poor, with a 5-year survival rate of less than 45%.
Grossly, SDC are grey-white and infiltrative, with the cut surface occasionally showing small cysts and areas of necrosis. The classic architecture resembles mammary intraductal carcinoma with tumor cells expanding salivary gland ducts with cribriform, “Roman-bridge,” solid and papillary patterns, frequently with central comedonecrosis. Mitoses, lymphovascular invasion, and perineural invasion are frequently present. An infiltrative component with a strong desmoplastic reaction is usually present. The neoplastic cells are cuboidal to polygonal with eosinophilic, granular cytoplasm and large, pleomorphic nuclei with coarse chromatin and prominent nucleoli. Cells may display luminal apical snouts. Variants include micropapillary, sarcomatoid, mucin-rich, and osteoclast giant-cell type. The tumor presented here shows prominent micropapillary architecture. The mucin-rich variant contains abundant mucin forming lakes that contain tumor islands. The sarcomatoid variant is a biphasic tumor, containing both classical architecture and a sarcomatoid component consisting of highly atypical spindled cells. The osteoclast giant-cell type contains osteoclast-like giant cells similar to giant cell tumor of bone.
SDC is positive for CK AE1/3, CK7, 34bE12, CEA, and EMA. It is negative for myoepithelial markers such as S100, CK5/6, p63, calponin, and SMMHC. PLAG1 and/or HMGA2 amplification is identified in most cases of SDC ex pleomorphic adenoma. It displays a similar immunohistochemical profile to breast cancer, with more than 80% of tumors staining positively for GCDFP15 and 67% to 83% staining positively for AR. Due to the high frequency of AR receptor positivity in salivary duct carcinomas and its near-absence in other salivary gland tumors, AR receptor positivity is frequently used to confirm the diagnosis. Like invasive mammary ductal carcinoma, HER2 amplification is seen in as many as 25% of cases, GATA3 tends to be positive and p53 can be overexpressed. However, unlike breast cancer, where greater than 75% of tumors are ER/PR positive, salivary duct carcinoma is rarely positive for ER/PR. PIK3CA mutations and PTEN loss have been observed in some cases with HER2 amplification, and it has been suggested that testing for these alterations be performed before starting trastuzumab therapy due to the potential reduced response rate.
Acinic cell carcinoma is the second most common malignant salivary gland tumor, and the mean patient age at presentation is 50 years old. It most commonly affects the parotid gland and usually presents as a well-circumscribed nodule. The neoplasm is composed of serous acinar cells with basophilic cytoplasm containing zymogen granules and hyperchromatic, round, eccentric, monomorphic nuclei, most commonly arranged in a lobular pattern. The granules are periodic acid Schiff (PAS)-positive and diastase-resistant. Acinic cell carcinomas rarely show mitoses and are usually a low- to intermediate-grade malignancy. SOX10 tends to be positive and EMA tends to be negative in acinic cell carcinoma, whereas SDC tends to be negative for SOX10. Acinic cell carcinoma is negative for GCDFP15 and AR.
Adenoid cystic carcinoma accounts for fewer than 10% of salivary gland tumors. The median age of diagnosis is 57 years, with a female-to-male ratio of 1.5:1. It most frequently occurs in the major salivary glands, but more than one-third of cases occur in minor glands. It is an infiltrative tumor composed of epithelial and myoepithelial cells with scant cytoplasm and angular nuclei forming cribriform, tubular, and/or solid structures. The most classic pattern is the cribriform pattern, which is composed of aggregates of basaloid cells interrupted by punched-out, sharply defined round spaces filled with lightly basophilic myxoid matrix and/or hyalinized stroma. Perineural invasion is characteristic. The epithelial cells are usually positive for KIT, while SMA and p63 highlight the myoepithelial cells. Adenoid cystic carcinomas are negative for GCDFP15 and are usually AR-negative. Many have a t(6;9) translocation resulting in a MYB::NFIB gene fusion.
Mucoepidermoid carcinoma (MEC) is the most common malignant salivary gland tumor and occurs most commonly in the parotid gland, affecting a wide age range. It is comprised of variable amounts of squamous, intermediate and mucin-producing cells with a cystic and solid growth pattern. There are various grading systems that have been applied to MEC, including the Armed Forces Institute of Pathology, Healey and Brandwein systems. Common to these systems is that low-grade mucoepidermoid carcinomas are predominantly cystic. Higher-grade MECs are less cystic and show necrosis, anaplasia, increased mitoses, and perineural or lymphovascular invasion. Mucoepidermoid carcinoma can be HER2-positive, but unlike salivary duct carcinoma, the epidermoid and intermediate cells are p63 positive. CK 5/6 highlights epidermoid-type cells. Mucoepidermoid carcinomas are usually negative for GCDFP15 and AR. Many contain a t(11;19)(q21;p13) translocation causing a CRTC1::MAML2 gene fusion. Tumors with the translocation and gene fusion tend to be of low to intermediate grade.
Secretory carcinoma (SC; previously known as mammary analog secretory carcinoma) usually presents in adults with a mean age of 46.5 years. It most commonly affects the parotid gland and presents as a poorly defined, rubbery mass. The tumor is comprised of microcystic, solid, tubular, follicular, and papillary-cystic structures with eosinophilic, bubbly secretions that are separated into lobules by fibrous septa. The tumor cells have eosinophilic, finely granular cytoplasm with small, uniform nuclei with vesicular chromatin and small nucleoli. SC can look similar to acinic cell carcinoma on H&E, but it lacks the secretory zymogen granules that give acinic cell carcinoma its positive PAS reaction. SC is usually positive for mammaglobin and S100 and is usually DOG1 negative, while acinic cell carcinoma is usually negative for mammaglobin and S100 and is usually DOG1 positive. SC can be positive for GATA3 and GCDFP15 but is negative for AR. SC contains a unique t(12;15)(p13;q25) translocation, which results in the fusion of the ETV6 and NTRK3 genes. FISH for this translocation is diagnostic.
Supplementary Questions
- Positivity for which of the following immunohistochemical stains favors a diagnosis of primary mammary invasive ductal carcinoma over secretory carcinoma of the salivary gland?
- AR
- ER
- GATA3
- GCDFP15
- p53
- Which of the following is true of salivary duct carcinoma?
- Comedonecrosis is frequently present.
- It is low- to intermediate-grade with a favorable prognosis.
- The neoplastic cells are basophilic and contain zymogen granules.
- The tumor cells are positive for PAS with diastase.
- The tumor cells contain small, uniform nuclei with vesicular chromatin.
- Which of the following genetic alteration is characteristic of secretory carcinoma of the salivary gland?
- 1p and 6q loss
- CRTC1::MAML2 gene fusion
- ETV6::NTRK3 gene fusion
- HER2 amplification
- MYB::NFIB gene fusion
References
- Butler RT, Spector ME, Thomas D, McDaniel AS, McHugh JB. An Immunohistochemical Panel for Reliable Differentiation of Salivary Duct Carcinoma and Mucoepidermoid Carcinoma. Head Neck Pathol. 2014;8(2):133-140.
- El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ, eds. WHO Classification of Head and Neck Tumours. 4th edition. IARC. 2017:163-178.
- Nasser SM, Faquin WC, Dayal Y. Expression of Androgen, Estrogen, and Progesterone Receptors in Salivary Gland Tumors. Frequent Expression of Androgen Receptor in a Subset of Malignant Salivary Gland Tumors. Am J Clin Pathol. 2003;119(6):801-806.
- Roh JL, Lee JI, Choi SH, et al. Prognostic factors and oncologic outcomes of 56 salivary duct carcinoma patients in a single institution: High rate of systemic failure warrants targeted therapy. Oral Oncol. 2014;50(11):64-66.
- Skálová A, Stenman G, Simpson RHW, et al. The Role of Molecular Testing in the Differential Diagnosis of Salivary Gland Carcinomas. Am J Surg Pathol. 2018;42(2):11-27.
- Urano M, Nagao T, Miyabe S, Ishibashi K, Higuchi K, Kuroda M. Characterization of mammary analogue secretory carcinoma of the salivary gland: discrimination from its mimics by the presence of the ETV6-NTRK3 translocation and novel surrogate markers. Hum Pathol. 2015;46(1):94-103.
- Zhu S, Schuerch C, Hunt J. Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Arch Pathol Lab Med. 2015;139(1):55-66.
Answer Key
- ER (b)
- Comedonecrosis is frequently present. (a)
- ETV6::NTRK3 gene fusion (c)