- Home
- Member Resources
- Pathology Case Challenge
- Peripancreatic Lymph Node
Clinical Summary
A 58-year-old woman presents with diarrhea. Esophagogastroduodenoscopy reveals multiple ulcers throughout the upper gastrointestinal tract, which were refractory to prior proton pump inhibitor treatment. Computed tomography scan shows duodenal and peri-pancreatic masses and regional lymphadenopathy. Laboratory studies show markedly elevated gastrin level. A peripancreatic lymph node is excised.
Master List of Diagnoses
- Hepatocellular carcinoma
- Metastatic papillary renal cell carcinoma
- Pancreatic solid pseudopapillary tumor
- Poorly differentiated neuroendocrine carcinoma (small cell carcinoma)
- Well-differentiated neuroendocrine tumor
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 13, and is well-differentiated neuroendocrine tumor in a peripancreatic lymph node.
Criteria for Diagnosis and Comments
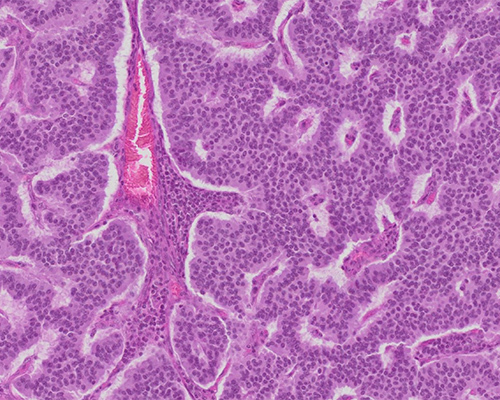
The diagnosis is well-differentiated neuroendocrine tumor (WNET), specifically G-cell neuroendocrine tumor (gastrinoma), which is the most common duodenal neuroendocrine tumor (NET). The slides show typical NET morphology including a crowded, monotonous population with centrally located round, ovoid nuclei, indistinct nucleoli, and moderate granular cytoplasm. The architecture of NET may be trabecular with pseudoglandular and pseudopapillary appearances, as in this case, but solid configuration is also common.
G-cell WNET is associated with H. pylori gastritis and long-term use of proton pump inhibitors. The term gastrinoma is not used for all tumors producing gastrin, only for those tumors producing clinical symptoms, such as diarrhea and refractory ulcers as in this case. G-cell WNET may occur in the stomach, ampulla, small intestine, or pancreas.
The World Health Organization (WHO) Classification of Tumours of Endocrine Organs (WHO 2017) classifies NET and carcinoma into four grades, dividing NETs into NET Grade 1 (G1), NET Grade 2 (G2), NET Grade 3 (G3), and small or large cell neuroendocrine carcinoma (NEC) Grade 3 (NEC G3). NET G1 and NET G2 are considered well-differentiated, however G3 may be well-differentiated or considered poorly differentiated neuroendocrine carcinoma.
WNET G3 was introduced in WHO 2017 because a subset of tumors that would have been classified as NEC on the basis of mitotic count and Ki-67 labeling index have less aggressive behavior, lower response to chemotherapy but better survival and lack genetic abnormalities of poorly-differentiated NEC. NET G3 retains well-differentiated morphology but shows a Ki-67 labeling index greater than 20% without an upper limit and typically, low expression of p53 by immunohistochemistry and mitotic count less than 20 per 10 high-power fields (HPF).
Except for gangliocytic paraganglioma and pancreatic neuroendocrine microadenomas, WHO 2017 categorizes all NET from the gastrointestinal and pancreaticobiliary tracts as malignant since all types are invasive cancers with the ability to metastasize to distant organs, as demonstrated by the current case, which showed metastases to regional lymph nodes.
Because increased tumor proliferation has been associated with an aggressive clinical course and poor prognosis, the current WHO 2017 classification system evaluates mitotic count and Ki-67 labeling index to determine NET grade as follows:
Differentiation |
Grade |
Mitotic Count per 10 HPF |
Ki-67 labeling Index, % |
Well-differentiated |
NET, G1 |
Less than 2 |
Less than 3% |
NET, G2 |
2 - 20 |
3-20% |
|
NET, G3 |
Greater than 20 |
Greater than 20% |
|
Poorly differentiated |
NEC, G3 |
Greater than 20 |
Greater than 20% |
- Small cell or large cell type |
|||
Tumor grade is determined without consideration of tumor size, extent, or location. Evaluation of tumor proliferation, both mitotic count and Ki-67 labeling, is determined from hot spots of activity. The mitotic count requires a minimum of 50 HPF and the Ki-67 labeling index requires evaluation of at least 500 cells. If a discrepancy is found between mitotic count and Ki-67 labeling index for tumor grade classification, then the higher grade should be used.
The current case mitotic activity is 4 per 10 HPF and the Ki-67 labeling index is 10%. Thus, this tumor is a NET, G2. Unlike the current case of NET, neuroendocrine carcinoma (NEC) typically shows brisk mitotic activity, apoptosis, and necrosis as features of its high proliferation, and morphologically, it is poorly differentiated and demonstrates sheets, ribbons or rosettes of small cells with minimal cytoplasm, and hyperchromatic nuclei with nuclear molding and smudging without distinct nucleoli.
The National Comprehensive Cancer Network (NCCN) recommends that the pathology report includes mitotic rate, Ki-67 labeling index, and tumor differentiation, as well as the grading system used. Clinicians view histologic grade as a general guide and use clinical judgment to make treatment decisions, particularly if the Ki-67, mitotic index, or differentiation classifications are discordant.
The current patient presented with multiple gastrointestinal ulcers, diarrhea, and gastric acid hypersecretion due to increased gastrin, and this triad of symptoms is characteristic of Zollinger-Ellison syndrome (ZES). Most cases of WNET are due to sporadic mutations; however, approximately 25%-40% of cases occur as part of the multiple endocrine neoplasia 1 (MEN1) syndrome.
Tumors that occur in patients with MEN1 are pituitary adenoma; parathyroid hyperplasia; and NETs of the pancreas, stomach, and duodenum. When ZES occurs in association with MEN1, the vast majority of responsible tumors are multifocal and located in the duodenum, as opposed to a pancreatic location. Tumors in patients with ZES and G-cell NET are frequently metastatic with unfavorable outcome, whereas MEN I-associated tumors typically occur at an earlier age and show benign clinical behavior. The current case demonstrates the typical behavior of ZES-associated NET, including low-grade cytology, low mitotic index, and multiple metastases.
Immunohistochemistry can be performed if clinically requested to determine specific cell types present in WNET, such as gastrin-, somatostatin-, glucagon-, vasoactive intestinal polypeptide (VIP)-, or insulin-producing cells. However, some microscopic morphology correlations exist. Somatostatinomas are classically associated with numerous psammoma bodies located within the glands; however, these are not specific to somatostatinomas and may occur in other WNET of the bowel and pancreas. Insulinomas typically show amyloid deposits. Clear cell tumors suggest von Hippel-Lindau syndrome, which is caused by germline mutations of the tumor suppressor gene VHL on chromosome 3p, with development of benign and malignant tumors affecting multiple organ systems.
Immunohistochemical studies for chromogranin and synaptophysin identify tumors of neuroendocrine origin and eliminate most other diagnostic considerations; however, some morphologic differences are present as well.
Metastatic hepatocellular carcinoma may show acinar architecture with pseudoglands and papillary-like formations, similar to NET. However, in most cases, hepatocellular carcinomas show at least focal areas of typical trabecular growth and cytology that shows more nuclear variation and abundant eosinophilic cytoplasm than is typical of WNET. Additionally, HepPar immunohistochemistry positivity would be consistent with metastatic hepatocellular carcinoma.
Metastatic papillary renal cell carcinoma, which may show low-grade nuclear features, may also be considered, particularly if the patient has a known history. Other features of papillary renal cell carcinoma include prominent stroma infiltration by neutrophils or foamy macrophages, psammoma bodies (type 1 papillary renal cell carcinoma), and PAX8 positivity.
Pancreatic solid pseudopapillary tumor (SPPT) may have solid and pseudopapillary components with low-grade ovoid nuclei and indistinct nucleoli. Additionally, synaptophysin and CD56 may be diffusely or focally positive in SPPT, but chromogranin is characteristically negative. SPPT shows progesterone receptor positivity and nuclear beta-catenin reactivity, which are unique and identifying features in this entity.
Supplementary Questions
- Which of the following is true in determining the proliferation rate and, thus, the grade in a well-differentiated neuroendocrine tumor (WNET)?
- If mitotic activity and Ki-67 are discordant for grade determination, the lowest grade should be used.
- Ki-67 index of 20% or greater classifies a WNET as grade 2.
- Mitotic activity and Ki-67 are evaluated in 10 high-power fields.
- Mitotic activity and Ki-67 are evaluated in hot-spot areas
- Regardless of mitotic activity and Ki-67 index, if metastases are present, the tumor is considered grade 3 neuroendocrine carcinoma.
- Which of the following immunohistochemical patterns would support pancreatic solid pseudopapillary tumor, differentiating it from WNET?
- Beta-catenin cytoplasmic staining
- CD56 (-)
- Estrogen receptor (+)
- Progesterone receptor (+)
- Synaptophysin (+)
- Which of the following is true?
- Amyloid deposition in a WNET is associated with von Hippel-Lindau syndrome.
- Determination of cell types present in a WNET may be elucidated from morphologic findings specific for a given cell type in combination with clinical syndrome present.
- H. pylori gastritis and long-term use of proton pump inhibitors are associated with WNET of the pancreas.
- MEN1-associated tumors typically are associated with multiple metastases and an aggressive clinical course.
- Zollinger-Ellison syndrome-associated WNET are frequently metastatic.
References
- Fletcher, C. Diagnostic Histopathology of Tumors. 4th ed. London, United Kingdom: Churchill Livingstone; 2013.
- Kim JY, Hong SM. Recent updates on neuroendocrine tumors from the gastrointestinal and pancreatobiliary tracts. Arch Pathol Lab Med. 2016;140(5):437–448.
- Lloyd RV, Osamura RY, Klöppel G, Rosai J, eds. WHO Classification of Tumours of Endocrine Organs. 4th ed. Lyons, France: IARC; 2017.
- Rosai J. Rosai & Ackerman's Surgical Pathology. 10th ed. Philadelphia, PA: Elsevier; 2011.
Author
Nichole L. Steidler, MD
Surgical Pathology Committee
Vista Pathology
Medford, OR
Answer Key
- Mitotic activity and Ki-67 are evaluated in hot-spot areas. (d)
- Progesterone receptor (+) (d)
- Zollinger-Ellison syndrome-associated WNET are frequently metastatic. (e)