- Home
- Member Resources
- Pathology Case Challenge
- Presacral Mass
Clinical Summary
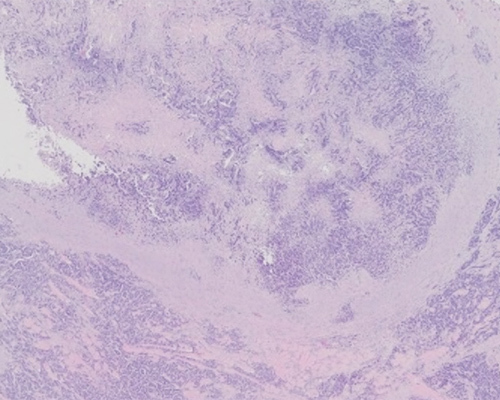
A 57-year-old man presents with complaints of difficulty urinating and bone pain. Imaging reveals a 5 cm presacral mass and pelvic lymphadenopathy. The tumor is composed of nests and sheets of epithelioid cells with prominent nucleoli. The tumor cells are positive for pankeratin and NKX3.1 but negative for GATA3, synaptophysin, FLI1, and SOX10.
Master List of Diagnoses
- Ewing sarcoma/peripheral neuroectodermal tumor
- Metastatic melanoma
- Metastatic pancreatic mixed ductal-neuroendocrine carcinoma
- Metastatic prostatic adenocarcinoma
- Metastatic urothelial carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 29, and is metastatic prostatic adenocarcinoma found in a pre-sacral mass.
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
The H&E-stained section shows areas of tumor with nested to sheet-like growth and focal gland formation, with suggestion of cribriform pattern in areas. The nuclei are relatively uniform, with prominent eosinophilic nucleoli. Immunohistochemical stains performed show that the tumor cells are positive for pankeratin, NKX3.1 and PSAP while negative for GATA3, SOX10, S100, synaptophysin, chromogranin, CD99, and FLI1. The patient’s laboratory workup reveals elevated serum prostate specific antigen (PSA) levels. This is most consistent with a diagnosis of metastatic prostatic adenocarcinoma.
Prostatic adenocarcinoma is the second most common cause of cancer-related death in men. It may be clinically suspected with elevated serum PSA and/or with an abnormal digital rectal exam. Clinical symptoms are rare in early-stage disease, but manifest in advanced disease with hematuria and/or bone pain.
The most common histologic type of prostatic adenocarcinoma is acinar adenocarcinoma. This type accounts for greater than 95% of prostate cancers. Acinar adenocarcinoma occurs predominantly in the posterolateral aspects (peripheral zone) of the prostate. Gross identification of prostatic carcinoma is often difficult, especially in small tumors. Larger tumors appear as indurated yellow homogenous nodules. Histologic examination shows glands with loss of surrounding basal cells. Acinar prostatic adenocarcinoma cells are cuboidal, with amphophilic to clear cytoplasm and prominent nucleoli. The lumen may contain blue mucin, eosinophilic amorphous secretions, and/or crystalloids. These findings are highly suggestive of prostatic adenocarcinoma, but not diagnostic. Pathognomonic features of carcinoma include circumferential perineural invasion, glomerulations, mucinous fibroplasia, and glands infiltrating adipose tissue.
Prostatic adenocarcinoma is graded using the Gleason system, which was developed by Dr. Donald Gleason in 1966. The Gleason score is a powerful predictor of the patient’s prognosis and also dictates the treatment that the patient will receive. The Gleason system uses histoarchitectural patterns to separate prostatic adenocarcinoma into five grades. Gleason grades 1 and 2 are no longer used in practice to grade prostatic adenocarcinoma. Gleason grade 3 consists of well-formed individual glands or branching glands infiltrating through benign glands. Gleason grade 4 consists of poorly formed or fused glands. Cribriforming and glomeruloid features are considered Gleason grade 4. Gleason grade 5 includes solid growth, single infiltrative cells, cords of cells, or cases with comedonecrosis. The combined Gleason score is assigned by selecting the most predominant and the second most prevalent patterns. The Gleason score should be reported as a mathematical equation, eg, 4+3=7. In biopsies, if the lower-grade component is less than 5% of the tumor, it is not reported, but the higher-grade component is reported regardless of amount. The prognostic grade group is assigned based on the combined Gleason score and should be reported along with Gleason score in all biopsy and resection specimens (Table 1). In general, it is not recommended to grade metastatic prostatic adenocarcinoma.
Table 1. Prognostic grade group
Gleason score 6 | Grade group 1 |
Gleason score 7 (3+4) | Grade group 2 |
Gleason score 7 (4+3) | Grade group 3 |
Gleason score 8 | Grade group 4 |
Gleason score 9-10 | Grade group 5 |
Extraskeletal Ewing sarcoma/Primitive neuroectodermal tumor (PNET) is an aggressive small round blue cell tumor seen primarily in adolescents and young adults. It occurs predominantly in the deep soft tissue of the extremities and paravertebral soft tissue (less commonly). The tumor is histologically composed of solid sheets of densely packed cells with round uniform nuclei and scant cytoplasm. The nuclei have dispersed fine chromatin and inconspicuous nucleoli. Homer Wright rosettes, which can be mistaken for glands, may be seen. These tumors characteristically show a strong diffuse membranous staining for CD99 and nuclear positivity for FLI1. Multiple balanced translocation and fusions involving the EWSR1 gene on chromosome 22 have been described, t(11;22)(q24;q12) being the most common. For this case, PNET would be an unlikely diagnosis, as it generally presents in much younger patients.
Melanoma can metastasize to any location and can show a wide variety of morphologic appearances. The hallmark finding is the presence of cells with marked cytologic atypia, prominent nucleoli and cytoplasmic melanin pigment. Although helpful, these hallmark findings may not be present in all cases of metastatic melanoma. Other histologic features encountered in metastatic sites can include epithelioid, spindle cell, pleomorphic, rhabdoid, signet ring, and small cell features. The small cell variant presents as a sheet of monotonous small round cells with hyperchromatic nuclei, inconspicuous nucleoli, and scant cytoplasm. Immunohistochemical stains are a helpful tool to help distinguish metastatic melanoma from other tumors. Melanocytic markers, such as S100, SOX10, MITF, HMB45, MelanA, and tyrosinase, are helpful. In this case, the presence of pankeratin and NKX3.1 expression and lack of SOX10 expression in tumor cells argue against the diagnosis of metastatic melanoma.
Neuroendocrine neoplasms of the pancreas are categorized by the 2017 World Health Organization as well-differentiated pancreatic neuroendocrine tumors (PanNET), poorly differentiated pancreatic neuroendocrine carcinomas (PanNEC), and mixed neuroendocrine/non-neuroendocrine neoplasms (MiNEN). MiNEN are composed of typically a ductal adenocarcinoma or acinar cell carcinoma, along with a neuroendocrine component. Each component must be at least 30% of the neoplasm to count toward classification as a MiNEN. Immunohistochemical stains for neuroendocrine markers (eg, synaptophysin) would be positive in such a MiNEN, but the current case is negative for synaptophysin.
Urothelial carcinoma is the fourth most common cancer in men in the United States. It is more common in men than women, with a median age of 65 - 70 years; the risk increases by 2.5 times for smokers. Urothelial carcinoma can be divided into flat, non-invasive, and invasive neoplasms. Flat lesions include urothelial carcinoma in situ. Non-invasive lesions include low- and high-grade papillary urothelial carcinoma. Invasive urothelial carcinoma may have divergent differentiation to show glandular, squamous, or neuroendocrine features. The histologic subtypes of invasive urothelial carcinoma with worse prognosis are micropapillary, sarcomatoid, plasmacytoid, lymphoepithelioma-like, and undifferentiated carcinoma. Helpful markers to distinguish urothelial carcinomas in metastatic sites include GATA3, uroplakin, and thrombomodulin. In the current case, tumor cells are negative for GATA3, favoring the diagnosis of prostate carcinoma over urothelial carcinoma.
Supplementary Questions
- Which of the following is true regarding prostatic adenocarcinoma?
- Gleason score is a powerful predictor of outcome in patients with prostatic adenocarcinoma.
- Glomeruloid features are graded as Gleason pattern 5.
- It is the most common cause of cancer-related death in men.
- Prostatic adenocarcinomas show staining with FLI1.
- Treatment options mainly depend on the serum PSA levels.
- Which of the following is true regarding prostatic adenocarcinoma?
- Circumferential perineural invasion is a feature of malignant prostatic glands.
- Glomerulation is not a feature of malignant prostate glands.
- In biopsies, both lower- and higher-grade components are reported regardless of amount.
- Mucinous adenocarcinoma is the most common histologic subtype of prostate carcinoma.
- The presence of crystalloids is considered pathognomonic for malignant prostatic glands.
- Which of the following is true regarding extraskeletal Ewing sarcoma/Primitive neuroectodermal tumor?
- Homer Wright rosettes are always present.
- It mainly occurs in elderly patients.
- It occurs primarily in superficial soft tissue of head and neck area.
- The most common translocation is the t(11;22)(q24;q12) :: (EWSR1::FLI1) fusion.
- These tumors show strong diffuse membranous staining for FLI1 and nuclear positivity for CD99.
References
- Blessing K, Grant JJH, Sanders DSA, Kennedy MM, Husain A, Coburn P. Small cell malignant melanoma: a variant of naevoid melanoma. Clinicopathological features and histological differential diagnosis. J Clin Pathol. 2000;53(8):591-595.
- Goldblum JR, Folpe AL, Weiss SW (eds) Enzinger & Weiss's Soft Tissue Tumors, Sixth Edition., Elsevier Saunders Health Sciences, 2014, Ch 33, Malignant Soft Tissue Tumors of Uncertain Type pp. 1028–1112.
- Gordetsky J, Epstein J. Grading of prostatic adenocarcinoma: current state and prognostic implications. Diagn Pathol. 2016;11:25,1-8.
- Grignon DJ, et al. Tumors of the Urinary Tract in: Moch H, Humphrey PA, Ulbright TM, Reuter, VE (eds). WHO Classification of Tumours of the Urinary System and Male Genital Organs,.4th Edition, IARC Press, 2016, pp. 81–107.
- Kloppel, G, et al. Neoplasms of the Neuroendocrine Pancreas. in: Lloyd RV, Osamura RY, Kloppel G, Rosai J (eds). WHO Classification of Tumours of Endocrine Organs, 4th Edition, IARC Press, 2017, pp. 211–214.
- Wang W, Epstein JI. Small cell carcinoma of the prostate. Morphologic and immunohistochemical study of 95 cases. Am J Surg Pathol. 2008;32(1):65-71.
Answer Key
- Gleason score is a powerful predictor of outcome in patients with prostatic adenocarcinoma. (a)
- Circumferential perineural invasion is a feature of malignant prostatic glands (a)
- The most common translocation is the t(11;22)(q24;q12) EWSR1::FLI1 fusion. (d)