- Home
- Member Resources
- Pathology Case Challenge
- Retroperitoneum
Clinical Summary
A 70-year-old woman presents with increasing abdominal girth, discomfort, and bilateral leg swelling over several months. She also reports a weight gain of 60 lbs during this period, early satiety, and decreased appetite. Radiologic studies show a large abdominopelvic/retroperitoneal mass measuring 34 cm in greatest dimension and compressing the inferior vena cava. The resected mass weighs 17 kilograms and displays a lobulated yellow cut surface.
Master List of Diagnoses
- Myxoid liposarcoma
- Pleomorphic liposarcoma
- Renal angiomyolipoma
- Well-differentiated liposarcoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 08, and is well-differentiated liposarcoma in the retroperitoneum.
Criteria for Diagnosis and Comments
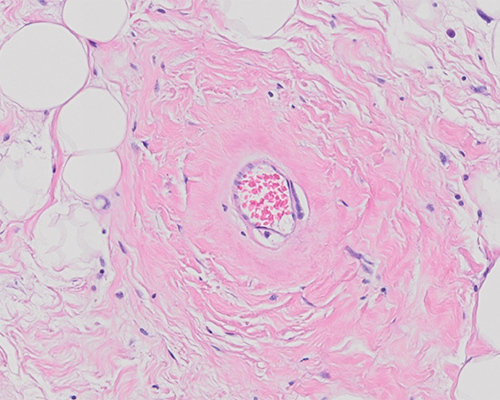
Histologic sections show relatively mature adipocytes of varying size, some of which contain atypical and hyperchromatic nuclei. Interspersed fibrotic bands containing scattered spindle and multipolar stromal cells with hyperchromatic nuclei are present. Depending on the area sampled, varying numbers of univacuolated and multivacuolated lipoblasts are identified. These findings are consistent with well-differentiated liposarcoma (WD-LPS).
Atypical lipomatous tumor/well-differentiated liposarcoma (ALT/WD-LPS) is a locally aggressive neoplasm that presents as a deep-seated painless enlarging mass that can grow slowly to attain a very large size. These tumors occur in middle-aged adults with peak incidence in the sixth decade, with equal distribution in males and females. The most common sites of involvement are the deep soft tissues of the limbs, especially the thigh, followed by the retroperitoneum, the paratesticular area, and the mediastinum. Retroperitoneal tumors are often asymptomatic until the tumor has exceeded 20 cm in diameter.
The term "well-differentiated liposarcoma" is used almost exclusively for tumors arising in the retroperitoneum, mediastinum, and pelvis, while the term "atypical lipomatous tumor" is used for those arising in the extremities. They are identical morphologically, karyotypically, and in terms of biologic behavior. However, retroperitoneal tumors are associated with a higher rate of recurrences largely due to difficulty in obtaining clear margins surgically.
On gross examination, WD-LPS is typically a large, well-circumscribed lobulated mass, with yellow to white firm cut surface depending on the proportion of mature adipocytic, fibrotic, and myxoid areas. Areas of fat necrosis are typical of large tumors. Histologically, WD-LPSs are composed predominantly of mature adipocytes showing significant variation in cell size and at least focal nuclear atypia. Scattered hyperchromatic and multinucleated stromal cells and varying numbers of lipoblasts are often present. Historically, WD-LPSs have been divided into lipoma-like, sclerosing, and inflammatory subtypes but the presence of more than one morphologic pattern is common, particularly in the retroperitoneal tumors. The characteristic MDM2 and CDK4 gene amplification on chromosome 12 seen in nearly all WD-LPSs can be highlighted with FISH studies. Immunohistochemistry can also be used as an adjunct tool with overexpression of the corresponding proteins manifesting as nuclear positivity.
Surgical resection with clear and wide margins is the treatment of choice for WD-LPS. The most important prognostic factor is the anatomic location; tumors occurring in surgically amenable sites such as soft tissue of the extremities have low rates of recurrence following complete excision with clear margins while those occurring in deep anatomic sites such as retroperitoneum tend to recur repeatedly and may result in death due to local effects or dedifferentiation and potential metastases.
The term “dedifferentiation” is applied when a lipogenic tumor shows progression either in the primary or subsequent recurrence to a higher grade sarcoma with no obvious morphologic line of differentiation. The risk of dedifferentiation varies with size, location, and duration of the pre-existing tumor, but overall the estimated frequency of dedifferentiation is 10% with > 20% reported for retroperitoneal tumors. The overall mortality for WD-LPS ranges from 0% for atypical lipomatous tumor of the extremities to > 80% for those of retroperitoneum in patients followed for 10 to 20 years.
Myxoid liposarcoma (MLS) makes up approximately 5% to 10% of sarcomas and tends to occur in younger patients. MLS is most commonly located in the deep soft tissues of the extremities and is very rarely seen in the retroperitoneum. Most MLS are relatively paucicellular with abundant myxoid background with a rich capillary network, often assuming a “pulmonary edema” pattern. The low-power vascular pattern sets MLS apart from other myxoid tumors. While the cellularity is relatively low, the cells that are present tend to be small, round with minimal mitotic activity. In addition, there are usually numerous lipoblasts. The presence of a prominent vascular pattern is helpful in differentiating MLS from dedifferentiated LPS with myxoid change. In addition, the majority of MLSs are characterized by a FUS-DDIT3 gene fusion, a feature that can be exploited for diagnostically difficult cases.
Pleomorphic liposarcoma (PLS) is the rarest subtype accounting for about 5% of all liposarcomas and occurs most commonly in the extremities while the trunk, retroperitoneum and spermatic cord are less frequently affected. Histologically, PLS has infiltrative margins and contain a varying number of lipoblasts in a background of a high-grade pleomorphic sarcoma. The presence of lipoblasts is essential for diagnosis highlighting the importance of adequate sampling. In most cases, the non-lipogenic component resembles undifferentiated pleomorphic sarcoma with spindle and multinucleated giant cells some of which are extremely large and often contain clear or vacuolated cytoplasm. The cytogenetic profile of PLS resembles those of other pleomorphic sarcomas rather than that of WD-LPS/dedifferentiated LPS.
Renal angiomyolipoma (AML) belongs to the family of perivascular epithelioid cell tumors (PEComas) and presents as a yellow to gray mass varying in size from a few centimeters to 20 cm or more. The mass is usually well-delineated from the adjacent renal parenchyma. Microscopically, AML is composed of 3 tissue elements varying greatly: mature adipose tissue, thick-walled convoluted blood vessels, and sheets and interlacing bundles of smooth muscle often with a perivascular arrangement. The smooth muscle of AML expresses HMB45 in addition to actin and desmin. Tumors with a prominent fatty component may be mistaken for liposarcoma; however, the presence of thick-walled convoluted blood vessels and reactivity for HMB45 allow for their distinction.
Supplementary Questions
- Which of the following is most distinctive of well-differentiated liposarcoma (WD-LPS)?
- FUS-DDIT3 gene fusion
- Immunoreactivity for HMB45
- MDM2 gene amplification
- Thick-walled convoluted blood vessels
- Translocations involving chromosome 12
- Which of the following is true of WD-LPS?
- Dedifferentiation results in a distinct change in the cytogenetic profile.
- Distant metastases are common.
- Prognosis is independent of anatomic location.
- Surgical resection with clear margins is the treatment of choice.
- Tumors occurring in the extremities have higher rate of recurrence.
- Which of the following is most typical of pleomorphic liposarcoma?
- Areas of WD-LPS at the periphery
- CDK4 gene amplification on chromosome 12
- Hypocellularity with prominent myxoid background with a rich capillary network
- Non-lipogenic component resembling undifferentiated pleomorphic sarcoma
- Well-circumscribed margins histologically
References
- Crago A, Singer S. Clinical and molecular approaches to well-differentiated and dedifferentiated liposarcoma. Curr Opin Oncol. 2011; 23(4):373–378.
- Matthyssens LE, Creytens D, Ceelen WP. Retroperitoneal liposarcoma: current insights in diagnosis and treatment. Front Surg. 2015;2:4:1-20.
- Mavrogenis AF, Papagelopoulos PJ. Well-differentiated liposarcoma. Atlas Genet Cytogenet Oncol Haematol. 2013;17(8):579-582.
- Sbaraglia M, Dei Tos AP, Pedutour F. Atypical lipomatous tumour/well-differentiated liposarcoma. In: WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours: WHO Classification of Tumours, 5th ed. IARC press; 2020:33-43.
- Vijay A, Ram L Retroperitoneal liposarcoma: a comprehensive review. Am J Clin Oncol. 2015;38(2):213-219.
- Ware PL, Snow AN, Gvalani M, Pettenati MJ, Qasem SA. MDM2 copy numbers in well-differentiated and dedifferentiated liposarcoma: characterizing progression to high-grade tumors. Am J Clin Pathol. 2014;141(3):334-341.
Author
Vijaya B. Reddy, MD
Surgical Pathology Committee
Rush University Medical Center
Chicago, IL
Answer Key
- MDM2 gene amplification (c)
- Surgical resection with clear margins is the treatment of choice. (d)
- Non-lipogenic component resembling undifferentiated pleomorphic sarcoma (d)