- Home
- Member Resources
- Pathology Case Challenge
- Retroperitoneum
Clinical Summary
A 25-year-old man presents for follow up of a testicular mass, status post orchiectomy 8 months ago. He is currently on chemotherapy. A computed tomography scan demonstrates a large periaortic mass in the lower abdomen. The excised tumor is 11 cm, partially encapsulated with a bosselated surface. Sectioning discloses soft, tan tissue, interspersed with innumerable discrete cysts filled with turbid, watery fluid, or coagulated white material that are up to 0.7 cm in size. Beta-human chorionic gonadotropin (β-hCG) and alpha fetoprotein (AFP) are within normal limits.
Master List of Diagnoses
- Metastatic adenosquamous carcinoma of the pancreas
- Metastatic mixed germ cell tumor
- Metastatic teratoma, consistent with growing teratoma syndrome
- Peritoneal keratin granuloma
- Primary teratoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2020, Case 32, and is metastatic teratoma, consistent with growing teratoma syndrome in the retroperitoneum.
The information provided in this case was accurate and correct at the time of publication in 2020.
Any changes in terminology since the time of publication may not be reflected in this case.
Criteria for Diagnosis and Comments
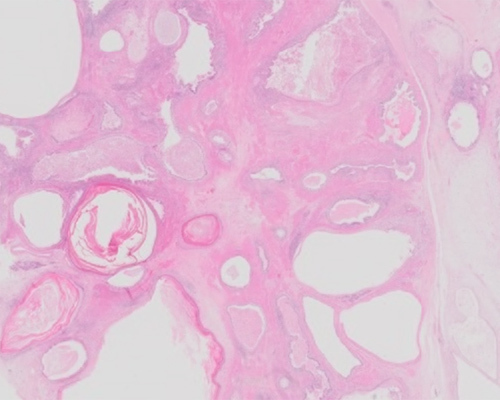
Sections show predominantly ectodermal and endodermal elements in the form of keratinous cysts with occasional dermal adnexa and cysts lined by respiratory or gastrointestinal epithelium. The cysts are frequently ruptured with resultant chronic inflammation and foreign body reaction. Additional sections show foci of cartilaginous (mesodermal) differentiation. No malignant degeneration is seen. The histologic appearance is consistent with teratoma, and given the context of a prior testicular tumor, a diagnosis of a metastatic teratoma, consistent with growing teratoma syndrome (GTS) is appropriate.
While most masses that appear during or after treatment of nonseminomatous germ cell tumors (NSGCT) are recurrences of the original tumor, rarely these masses can represent GTS. GTS affects patients with a history of NSGCT and is characterized by increasing size of metastatic lesions during or after systemic chemotherapy in the setting of normalized serum tumor markers. By definition, GTS includes (1) normalization of the serum tumor markers (alpha fetoprotein [AFP] and beta-human chorionic gonadotropin [β-hCG]) (2) enlarging or new masses despite appropriate chemotherapy for NSGCT; and (3) only mature teratoma on pathologic examination, with no other viable germ cell components, such as seminoma or other variants.
GTS is a rare entity, with an incidence of 2% to 8% after testicular NSGCT and 12% after ovarian germ cell tumors, occurring predominantly in young adults and adolescents. GTS is more likely to occur when the primary tumor contained teratomatous elements and when there is no or little reduction in size following chemotherapy or resection of the primary tumor. While the etiology remains unknown, there are two main hypotheses, the first being that chemotherapy selects for the benign teratomatous elements while curing the immature malignant germ cells. The second hypothesis is that chemotherapy alters the cellular kinetics toward transformation from a totipotent malignant germ cell toward a benign mature teratoma. The most common location for GTS is the retroperitoneum, but it has also been shown to occur in the lung, mediastinum and lymph nodes.
The histology is that of a teratoma with ectodermal, mesodermal, and endodermal elements represented. For example, cartilage, ciliated respiratory-type epithelium, enteric epithelium, and neurogenic tissue with a supporting stroma of undifferentiated mesenchymal spindle cells have been reported. Additionally, GTS may have solid and cystic features. Malignant transformation in a teratoma to squamous cell carcinoma, adenocarcinoma, sarcoma, primitive neuroectodermal tumor or carcinoid tumor has been reported in about 3% of cases.
While usually benign, there is significant morbidity and mortality associated with these tumors due to invasive and compressive growth. Thus, early detection and diagnosis is imperative. Treatment remains surgical resection, with only a few reported cases showing any benefit of post-resection chemotherapy or radiation therapy. While complete surgical resection is often curative, recurrence rates of 72% to 83% have been reported in patients with partial resections. The prognosis is generally good, with a 5-year overall survival rate of 89% in those who undergo surgery.
Differential diagnostic considerations depend on the location and differentiation of the tumor.
Adenosquamous carcinoma of the pancreas is a rare aggressive malignancy with dual differentiation toward adenocarcinoma and squamous carcinoma. This tumor is immunoreactive for pancytokeratin, CK5/6, CA19-9, and CEA, and variably reactive for CK7, Cam5.2, and CK20. The tumor typically arises in the head of the pancreas and has an average survival of 5.8 months after diagnosis. Most cases demonstrate KRAS mutation. The lack of malignant features makes this diagnosis unlikely.
Mixed germ cell tumors contain more than one germ cell tumor component, and in the testis, are much more common than any of the pure histologic forms. The order of frequency of histologic subtypes is as follows: embryonal carcinoma, teratoma, yolk sac tumor, seminoma, and choriocarcinoma. These tumors commonly metastasize to the retroperitoneal lymph nodes. About 10% of metastases occurring after chemotherapy demonstrate a nonteratomatous component. The differentiation of metastatic residual teratoma from nonteratomatous types is important as pure teratomatous metastasis is treated by surgical excision while other residual germ cell tumor components are treated with additional chemotherapy. The absence of other germ cell tumor subtypes in combination with normal serum markers precludes metastatic mixed germ cell tumor.
Primary teratoma of the retroperitoneum is rare and accounts for about 4% of all primary teratomas and 1% to 11% of all primary retroperitoneal neoplasms. This occurs more commonly in neonates, infants, and children. Retroperitoneal tumors in adults are more likely metastasis from the gonadal tissue than true primary tumors. When they occur, they usually arise in the upper portion of the left kidney. The rate of malignancy is 7% in children and 26% in adults. The overall 5-year survival is nearly 100% with complete surgical excision. Given the clinical history of a prior testicular tumor, a primary retroperitoneal teratoma is less likely.
Peritoneal keratin granuloma is a rare condition associated with endometrioid adenocarcinoma with squamous differentiation of the uterus and ovary and atypical polypoid adenomyoma. It is commonly seen in postmenopausal women and unlikely in men or other younger adults. Microscopically, it is composed of eosinophilic laminated keratin surrounded by multinucleate giant cells, histiocytes, lymphocytes, and plasma cells. It can be confused with disseminated carcinoma microscopically, as reactive mesothelial cells near the keratin granulomas can proliferate and form papillary or glandular structures. Viable carcinomatous cells are rarely found. The patient’s gender and absence of distinct keratin granulomas preclude this diagnosis.
Supplementary Questions
- Which of the following features is true about growing teratoma syndrome?
- Alpha fetoprotein and beta-human chorionic gonadotropin are elevated.
- Chemotherapy plays a significant role in treatment.
- Imaging studies do not assist with making the diagnosis.
- Malignant transformation is seen in a small percentage.
- They are frequently associated with seminoma.
- What is the most common site of presentation for growing teratoma syndrome?
- Liver
- Lung
- Mediastinum
- Pineal gland
- Retroperitoneum
- Which of the following scenarios is most consistent with peritoneal keratin granuloma?
- A 55-year old man presenting with jaundice
- A 40-year old man with a large retroperitoneal mass
- A post-menopausal woman presenting with uterine bleeding
- A 10-year old girl with a mass in the upper portion of the left kidney
- A 20-year old man with a history of testicular seminoma
References
- Boukettaya W, Hochlaf M, Boudagga Z, et al. Growing teratoma syndrome after treatment of a nonseminomatous germ cell tumor: A case report and review of the literature. Urol Case Rep. 2014;2(1):1-3.
- Kardon DE, Thompson LDR, Przygodzki RM, Heffess CS. Adenosquamous carcinoma of the pancreas: A clinicopathologic series of 25 cases. Mod pathol. 2001;14(5):443-451.
- Michael H, Lucia J, Foster RS, Albright TM. The pathology of late recurrence of testicular germ cell tumors. Am J Surg Pathol. 2000;24(2):257-273.
- Priod F, Lorge F, Di Gregorio M, et al. Recurrent masses after testicular cancer: Growing teratoma syndrome. A case report and review of the literature. Case Rep Oncol. 2017;10(3):910-915.
- Rentea R., Varghese A, Ahmed A, et al. Pediatric ovarian growing teratoma syndrome. Case Rep Surg. 2017;3074240:1-8.
- Sasi W, Ricchetti GA, Parvanti L, Carpenter R. Giant mature primary retroperitoneal teratoma in a young adult: Report of a rare case and literature review. Case Rep Surg. 2014;930538:1-5.
- Scavuzzo A, Santana Rios ZA, Noverón NR, Jimenez Rios MA. Growing teratoma syndrome. Case Rep Urol. 2014;139425:1-4.
- Tarrant WP, Czerniak BA, Geo CC. Relationship between primary and metastatic testicular germ cell tumors: a clinicopathologic analysis of 100 cases. Hum Pathol. 2013;44(10):2220-2226.
Answer Key
- Malignant transformation is seen in a small percentage. (d)
- Retroperitoneum (e)
- A post-menopausal woman presenting with uterine bleeding (c)

