- Home
- Member Resources
- Pathology Case Challenge
- Small Intestine
Clinical Summary
A 50-year-old man presents to the emergency department with diffuse abdominal pain. His abdomen is markedly tender to palpation with significant guarding. A computed tomography scan reveals pneumoperitoneum with free air within the bowel wall. A partial small bowel resection is performed. The resected small intestine is markedly dilated and easily compressible with palpable crepitus. On opening, multiple cysts are seen throughout the bowel wall, which quickly deflate following sectioning.
Master List of Diagnoses
- Crohn disease
- Lipomatosis
- Pneumatosis cystoides intestinalis
- Pseudolipomatosis
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 29, and is pneumatosis cystoides intestinalis, manifested in the small intestine.
Criteria for Diagnosis and Comments
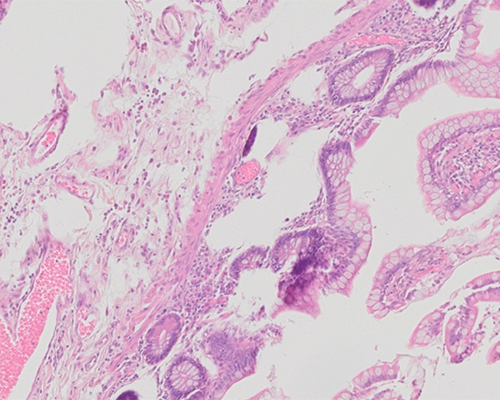
Sections of the intestine show attenuated but benign appearing epithelium. There are nonspecific architectural changes. The lamina propria shows a mild increase in lymphoplasmacytic cells. Granulomas are not seen. The submucosa demonstrates multiple large cystic spaces with nearby giant cells. These findings are consistent with pneumatosis cystoides intestinalis (PC).
PC is characterized by the presence of large, gas-filled cysts within the submucosa. These cysts are often best appreciated grossly. Following resection, the fresh specimen is often markedly dilated. However, as the cysts are filled with gas, the bowel is easily compressible. Some cysts may be smaller in appearance, but often remain palpable. The bowel wall is often thickened. The mucosa is variable (depending on if the patient has concomitant diagnoses) but may show ulceration. Endoscopically, these cysts may exist as singles or multiples. The cysts can be misinterpreted as a polyposis syndrome, as they can form sessile or pedunculated lesions.
In small biopsy specimens, the cysts frequently deflate and may be less visible microscopically. However, the presence of giant cells or macrophages surrounding attenuated epithelium can aid in the diagnosis. Early cysts may show a thin lining akin to lymphatics, but often retain the closely approximated giant cells. Small cysts may also be seen in the lamina propria. These cysts, termed pseudolipomatosis (PL), show a very rounded appearance mimicking mature adipose tissue. PL cysts fail to show an epithelial lining and tend to “infiltrate” around the glands without forming a discrete nodule microscopically. PL is not exclusive to PC and may be seen as an incidental finding secondary to insufflation during colonoscopy.
PC can occur anywhere in the small or large intestine but is most common in the colon. Two forms of the disease occur: a less common and more dramatic form occurs in children, while the more common, indolent type is seen in adults. The majority of cases of PC are associated with entities that result in mucosal compromise. In children, PC is most commonly associated with necrotizing enterocolitis and fulminant inflammatory bowel disease. These coexisting diseases attest to the severe nature of PC in children. In adults, PC occurs in a variety of milieus, including inflammatory etiologies (eg, inflammatory bowel disease, infectious colitis, pseudomembranous colitis, appendicitis, or diverticulitis), intrinsic bowel abnormalities (eg, diverticulosis, sigmoid volvulus, or pyloric stenosis), pulmonary disease (eg, chronic obstructive pulmonary disease, asthma, cystic fibrosis, or emphysema), iatrogenic causes (eg, endoscopy with or without biopsy), connective tissue diseases, autoimmune diseases, chemotherapy, drugs, or trauma.
Approximately 85% of PC has a proximate cause, with the remaining presenting without a definite etiology. Multiple theories have been suggested to explain the cause of the cysts. One theory purports that mucosal injury allows for bacteria to colonize the submucosa, and while there, the bacteria produce gas that distends the bowel wall forming cysts. Another theory suggests that pressure within the gastrointestinal lumen causes fissures within the bowel wall allowing gas from digesting foods to track in. The final theory suggests ruptured blebs in pulmonary disease can allow air to pass down retroperitoneal vessels to the bowel wall. As each of these theories cannot explain every case of PC, it is likely that multiple etiologies result in a similar histologic appearance.
Clinically, patients with PC can be asymptomatic. The most common presenting symptom, however, is abdominal distention. Diarrhea or constipation may be present. The stool may contain blood or mucus. Severe cases may result in obstruction, hemorrhage, or perforation. As the cysts increase in size, adjacent abdominal structures may be compressed. These changes can sometimes be seen on X-ray or computed tomography scan.
Patients are often treated with supportive measures including decompression, bowel rest, parenteral nutrition, and fluid/electrolyte supplementation. Antibiotics are often used. Additionally, patients have been shown to benefit from hyperbaric oxygen and elemental diets. PC has a very favorable prognosis, with a significant number of patients showing spontaneous resolution without treatment. It may be several months before resolution occurs.
The differential diagnosis of PC is limited. The most likely process to be confused with this entity is Crohn disease (CD). The presence of numerous giant cells within the submucosa may resemble a granulomatous process, particularly when the specimen is a small biopsy and cysts deflate causing the giant cells surrounding the cysts to form aggregates resembling poorly formed granulomas, suggestive of CD. When multiple giant cells are encountered on a biopsy specimen, it is important that the specimen is thoroughly examined with multiple levels evaluated. The deflated cysts may be difficult to visualize, but can be seen as thin, angulated spaces which are surrounded by the giant cells in question. Unfortunately, CD can result in PC, further complicating the diagnosis. Equivocal cases are possible and should be followed clinically for additional signs of CD. Resection specimens tend to pose less of a diagnostic difficulty, but require careful scrutiny to identify concomitant disease, if present.
As mentioned previously, pseudolipomatosis should also be considered in the differential of PC. Although PL can be seen in PC, PL most commonly occurs as a result of insufflation during endoscopy. Gas becomes trapped within the lamina propria and forms rounded spaces akin to mature adipose tissue. In PL, there is rarely an infiltration of giant cells. The cysts tend to be smaller and limited to the lamina propria. Distinguishing PL from PC on biopsy is important, as the diagnosis of PC warrants searching for the cause, while PL is procedure related artifact. PL commonly spontaneously resolves without treatment.
Although less commonly encountered, multiple lipomas may be seen within the small intestine. Termed lipomatosis, multiple lipomas may be present throughout the small intestine mimicking the gross and microscopic appearance of PC. Grossly, the conditions may be differentiated by the lack of crepitus in lipomatosis. Microscopically, individual lipomas in lipomatosis have a typical histology seen in lipomas at other sites generally lacking giant cells and large cystic spaces
Supplementary Questions
- Which of these best describes the clinical characteristics of pneumatosis cystoides intestinalis?
- Abdominal distension is the most common symptom.
- An indolent form occurs commonly in children.
- It frequently requires surgery as treatment.
- It most commonly presents as an isolated phenomenon without an identifiable cause.
- Patients are most often younger than 20 years old.
- Which of the following is most helpful in differentiating Crohn disease from pneumatosis cystoides intestinalis on a biopsy?
- Capillary thrombosis
- Giant cells
- Lamina propria cysts
- Mucosal ulceration
- Well-formed granulomas
- A colon biopsy comes to your desk with the endoscopic impression of 4 mm elevated yellow plaques. Microscopically, you see a slightly attenuated colonic mucosa with small round clear structures infiltrating within the lamina propria. These rounded spaces do not appear to have lining cells. No giant cells or granulomas are seen. Macrophages are inconspicuous. Epithelial atypia is not seen. There is no significant architectural change within the crypts.
What is the most likely diagnosis?
- Crohn disease
- Juvenile (retention) polyp
- Lipoma
- Pneumatosis cystoides intestinalis
- Pseudolipomatosis
References
- Azzaroli F, Turco L, Ceroni L, et al. Pneumatosis cystoides intestinalis. World J Gastroenterol. 2011;17(44):4932-4936.
- Gebeoes K, Riddell R, Jain D. Inflammatory Bowel Diseases. In Riddell R, Jain D, eds. Lewin, Weinstein, and Riddell’s Gastrointestinal Pathology and Its Clinical Implications. Philadelphia, PA: Lippincott, Williams & Wilkins;2014:983-1208.
- Koreishi A, Lauwers GY, Misdraji J. Pneumatosis intestinalis: a challenging biopsy diagnosis. Am J Surg Pathol. 2007;31(10):1469-1475.
- Odze RD and Goldblum JR. Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas. Philadelphia, PA: Saunders;2015.
- Petras RE and Gramlich TE. Non-neoplastic Intestinal Disease. In Mills SE, ed. Sternberg’s Diagnostic Surgical Pathology. Philadelphia, PA: Lippincott, Williams, & Wilkins;2010:1313-1367.
- Shepherd NA, Warren BF, Williams GT, Greenson JK, Lauwers GY, Novelli MR. Morson and Dawson’s Gastrointestinal Pathology. West Sussex, UK: Wiley;2013.
- Wu LL, Yang YS, Dou Y, Liu QS. A systematic analysis of pneumatosis cystoids intestinalis. World J Gastroenterol. 2013;19(30):4973-4978.
Author
J. Clint Stanfill
Gastrointestinal Pathology Fellow
AmeriPath Cleveland
Cleveland, OH
Answer Key
- Abdominal distension is the most common symptom (a)
- Well-formed granulomas (e)
- Pseudolipomatosis (e)