Clinical Summary
A 68-year-old man with a three-week history of abdominal discomfort presents to the emergency department. Ultrasound reveals a massively enlarged spleen—the edge is approximately 12 cm below the costal margin. No lymphadenopathy is seen.
Concurrently performed CBC shows lymphocytosis. Peripheral blood smear examination shows abnormal lymphocytes with cytoplasmic polar projections. A manual differential shows that these lymphocytes comprise 36% of the white blood cells. An emergency abdominal splenectomy is performed. The spleen weighs 1220 grams and measures 22 cm in greatest dimension with a dark purple and red capsule with signs of clotted blood and surface rupture. Sections reveal a central area of hemorrhage and several small nodules. Fresh tissue is submitted for flow cytometry, cytogenetics and molecular studies, and histologic examination.
Flow cytometry shows that 30% of lymphocytes are kappa restricted B-lymphocytes that are negative for CD5, CD11c, CD103, and CD10. Karyotype revealed a deletion in the long arm of chromosome 7 (del 7q). BRAF V600E mutation analysis is negative.
Master List of Diagnoses
- Classic Hodgkin lymphoma
- Hairy cell leukemia
- Hepatosplenic T-cell lymphoma
- Lymphoplasmacytic lymphoma
- Splenic diffuse red pulp small B-cell lymphoma
- Splenic marginal zone lymphoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 14, and is splenic marginal zone lymphoma (spleen).
Criteria for Diagnosis and Comments
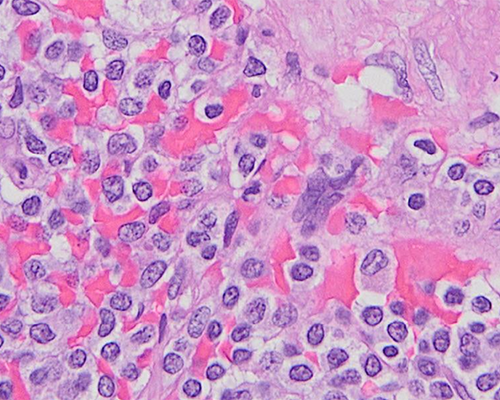
This patient with splenomegaly has peripheral blood lymphocytosis that shows polar villous lymphocytes. Flow cytometry reveals that the abnormal lymphocytes are clonal B cells that do not express aberrant antigens CD5 or CD10. Sections from the spleen show a congested red pulp and microscopic nodules (also observed on gross examination). The nodules represent abnormal white pulp effaced by small to intermediate-sized lymphocytes, which in some areas appear monocytoid with abundant cytoplasm. Many of the lymphocytes within the nodules show plasmacytoid differentiation. Immunostains show that these cells are positive for CD20 but negative for CD3, CD43, CD23, CD5, and CD10. Overall, the combined features are those of splenic marginal zone lymphoma (SMZL) (World Health Organization [WHO] 2017).
SMZL is a relatively rare B-cell neoplasm, presenting in adults over 50 years of age. Splenectomy for diagnosis is rarely performed currently since the diagnosis can be established by imaging and flow cytometry studies. About 30% of SMZLs show del 7q. Genomic profiling shows NOTCH2 is a frequently involved gene in SMZL. NOTCH2 mutations are also seen in other small B-cell lymphomas and, hence, do not have any additional value to distinguish SMZL from the other entities in the differential diagnosis, which are described below.
Classic Hodgkin lymphoma (CHL) can involve the spleen and can show nodules by gross examination. However, classic Hodgkin lymphoma contains large Hodgkin-Reed-Sternberg cells by histologic examination. Flow cytometry is typically negative in CHL. Even though recent studies have shown some genetic aberrations in CHL (by next generation sequencing), they do not overlap with SMZL.
Hairy cell leukemia is one of the chief differential diagnoses for SMZL. Both entities involve the spleen, can show peripheral blood involvement with abnormal lymphocytes showing cytoplasmic projections, and lack the aberrant antigens CD5 and CD10 by flow cytometry. The differentiating features of hairy cell leukemia include involvement of the red pulp of the spleen, circumferential fine projections of the peripheral blood lymphocytes, abnormal expression of CD11c, CD103, and CD25 by flow cytometry, and the presence of BRAF V600E mutation in most cases.
Hepatosplenic T-cell lymphoma (HSTL) is another lymphoma preferentially involving the spleen and frequently brought to attention because of massive splenomegaly and systemic symptoms. HSTL frequently show hepatic involvement. Splenic involvement is typically within the red pulp. This is a lymphoma with a poor prognosis.
Lymphoplasmacytic lymphoma (LPL) seldom involves the spleen, but when it does, it is frequently seen involving the white pulp; it can show a nodular or diffuse pattern. LPL is a peripheral blood and bone marrow centric disease and classically shows IgM monoclonal gammopathy detected by serum protein electrophoresis and serum immunofixation. LPL frequently has MYD88 mutation, which is not typically seen in SMZL.
Per the 2017 WHO guidelines, any splenic small B-cell lymphomas that do not fit in other categories of B-cell lymphoma involving the spleen can be categorized as splenic B-cell lymphoma/leukemia unclassifiable; this category includes splenic diffuse red pulp small B-cell lymphoma (SDRPL). This is, as the name implies, a dominantly red pulp disease and should not show nodules by gross or microscopic examination. SDRPL is a provisional entity which is not well characterized; however, this entity has more in common with hairy cell leukemia than SMZL.
SMZL is an indolent disease with long survival. Splenectomy with a curative intent is not performed, as hematologic response to rituximab-based regimen is favorable. Transformation to diffuse large B-cell lymphoma occurs in approximately 10% of cases and is typically associated with fast progression and NOTCH2, KLF2, and TP53 mutations.
Supplementary Questions
- Which of the following is true regarding splenic marginal zone lymphoma (SMZL)?
- Almost all cases are of plasma cell origin.
- Almost all cases of SMZL are Epstein-Barr virus driven.
- Most cases are seen in adolescents.
- Prognosis is very bleak.
- SMZL lymphocytes are negative for CD5, CD10, and CD103.
- Which of the following is correct regarding SMZL?
- BRAF V600E mutation is seen in both SMZL and hairy cell leukemia.
- Del 7q is seen in about 30% of SMZL cases, but no specific driver genes are known.
- MYD88 mutation is seen in the vast majority of SMZL cases.
- NOTCH2 has been identified as the specific driver mutation in a majority of SMZL cases.
- TP53 mutation is associated with all SMZL cases and is useful diagnostically.
- Which of the following is characteristic for the histologic appearance of SMZL?
- Diffuse large areas of atypical small to medium-sized cells preferentially involving splenic sinusoids
- Diffuse sheets of medium-sized, atypical lymphocytes, which line blood lakes in the red pulp
- Large aggregates of small to medium-sized cells solely confined to the red pulp, with possible monocytoid or plasmacytoid morphology
- Nodules representing abnormal red pulp with pleomorphic large cells, irregularly shaped nuclei, and prominent eosinophilic nucleoli
- Nodules representing abnormal white pulp composed of small to intermediate sized lymphocytes with possible monocytoid or plasmacytoid morphology
References
- Arcaini L, Rossi D, Paulli M. Splenic marginal zone lymphoma: from genetics to management. Blood. 2016;127(17):2072-2081.
- Harmon CM, Smith LB. B-cell non-Hodgkin lymphomas with plasmacytic differentiation. Surg Pathol Clin. 2016;9(1):11-28.
- Piris MA, Onaindia A, Mollejo M. Splenic marginal zone lymphoma. Best Pract Res Clin Haematol. 2017;30(1-2):56-64.
- Swerdlow SH, Campo E, Harris NL, et al, eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. IARC press; 2017.
Authors
Amanda Kitson, MD
Surgical Pathology Resident
University of Michigan
Ann Arbor, MI
Rajan Dewar, MD, PhD, FCAP
Surgical Pathology Committee
University of Michigan
Ann Arbor, MI
Answer Key
- SMZL lymphocytes are negative for CD5, CD10, and CD103. (e)
- Del 7q is seen in about 30% of SMZL cases, but no specific driver genes are known. (b)
- Nodules representing abnormal white pulp composed of small to intermediate sized lymphocytes with possible monocytoid or plasmacytoid morphology (e)