- Home
- Member Resources
- Articles
- All the Colors, None of the Drama? A Practical Primer on Spectral Flow Cytometry in Clinical Settings
For decades, flow cytometry has occupied a central role in the diagnosis, classification, and disease monitoring in clinical pathology and particularly in hematopathology. As clinical scenarios have grown more complex, driven by expanding disease classifications, targeted therapies, and need for diagnostic precision, the demand for higher parameter flow cytometric assays has intensified. Conventional flow cytometry (CFC) has steadily evolved to accommodate these needs but is increasingly challenged by practical limits in multiplexing capacity and panel design. Spectral flow cytometry (SFC) is an evolution in the field of flow cytometry and can improve the efficiency and analytical resolution of immunophenotyping in appropriate applications.1–3 Unlike CFC, which uses optical filters along with dichroic mirrors to measure fluorescence in individual detectors, SFC captures the full emission spectrum of each fluorophore across the entire range of wavelengths and a broad array of detectors, followed by mathematical algorithms to resolve individual signals. This approach enables building high-parameter panels (often exceeding 30 markers) including antibodies with highly overlapping fluorochromes within a single tube. Importantly, this technological shift does not alter established diagnostic frameworks or interpretive principles; instead, it changes how fluorescence-based data is acquired and signals are separated, while having the potential to streamline workflows, reduce specimen and resource requirements, and improve resolution of cells and populations. This primer provides a practical, clinically oriented overview of SFC, focusing on how it differs from conventional approaches, where it offers meaningful advantages, and what considerations should inform its implementation in a clinical pathology laboratory.
What is Spectral Flow Cytometry?
In flow cytometry, fluorescently antibody- or dye-labeled cells or particles in suspension are hydrodynamically focused by the fluidics system and interrogated individually as they pass through one or a series of laser beams.4,5 Fluorescence and scatter signals are collected by an optical system, which directs emitted light toward detectors. These optical signals are then converted into electrical signals and processed computationally to generate quantitative measurements for each event. In CFC, individual fluorochromes are detected using optical filters and dichroic mirrors, which direct predefined wavelength bands to individual detectors (Figure 1). Overlap in emission spectra is common and causes spillover between channels. CFC addresses this by using mathematical correction for spectral spillover (termed "compensation") and by careful panel design and assay validation, including fluorescent antibody choices and optimization of reagents, voltage, and acquisition settings. This approach has proven robust for smaller or simpler panels but becomes increasingly challenging as the number of fluorochromes increases and spectral overlap becomes more difficult to resolve. In practice, this reduces the number of fluorochromes (or specific combinations) that can be reliably incorporated into a diagnostic panel. SFC in contrast captures fluorescence emissions across a continuous range of wavelengths using an array of detectors.1,3,6 Each fluorochrome is thereby represented by a characteristic emission pattern across all detectors, often referred to as "spectral signature." Mathematical algorithms then deconvolute these signatures (termed "unmixing") to estimate the contribution of each fluorochrome to the measured signal, creating a "spectral fingerprint" for each fluorochrome (Figure 1).
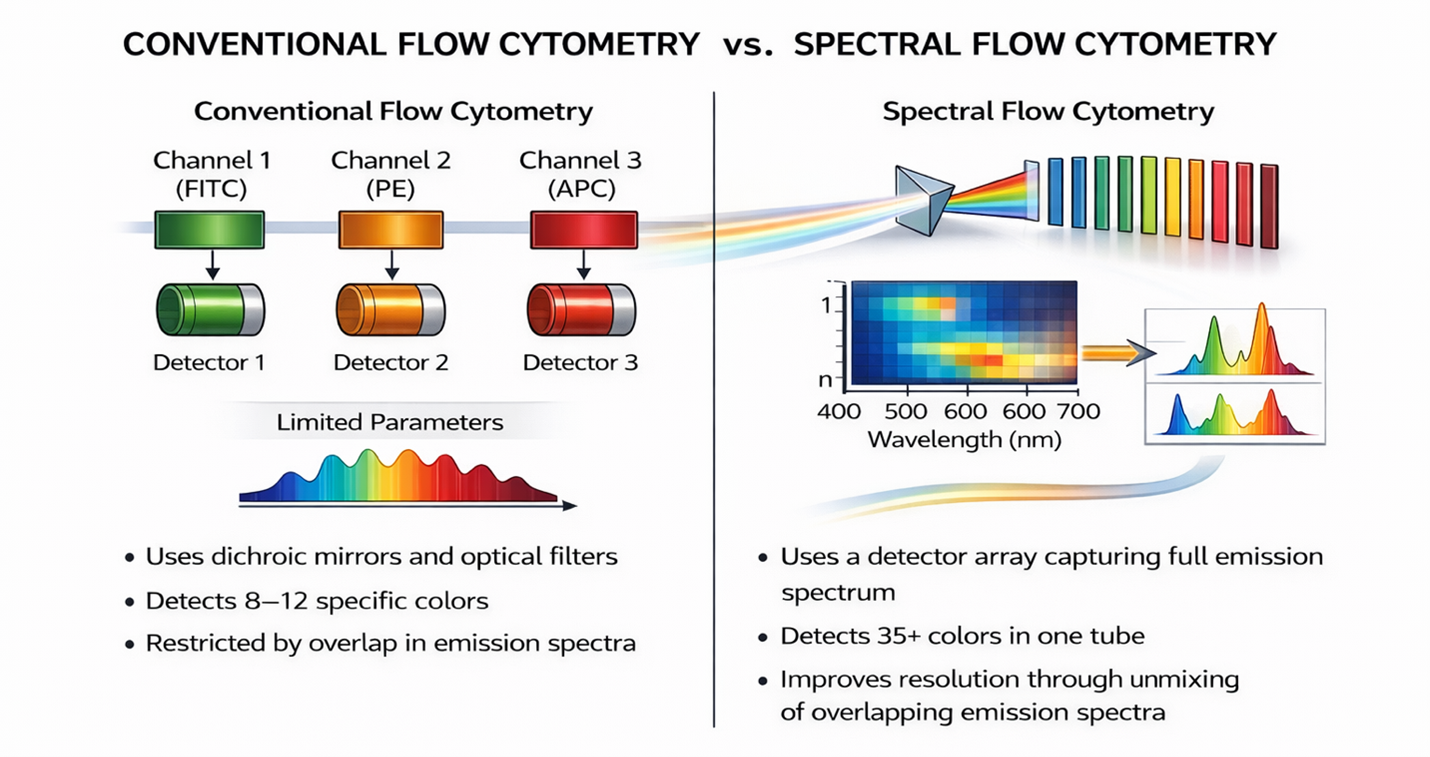
Figure 1: Conceptual comparison of conventional flow cytometry (CFC) and spectral flow cytometry (SFC). This simplified schematic illustrates the fundamental difference between discrete channel detection and full spectrum acquisition with computational signal separation. In CFC (left), emitted fluorescence is separated by optical filters and dichroic mirrors into discrete detection channels, each measuring a defined wavelength band corresponding to a specific fluorochrome (eg, FITC, PE, APC; note that substantially more fluorochromes and channels exist but are not shown for illustrative purposes). Because emission spectra overlap, signals must be corrected using compensation, and the number of fluorochromes that can be combined in a single panel is limited. In SFC (right), fluorescence emission across the full wavelength range is captured by a detector array, generating a spectral profile for each fluorochrome. Computational spectral unmixing then resolves overlapping signals based on their characteristic emission patterns, enabling the use of larger, higher parameter panels within a single tube and improving discrimination of closely overlapping fluorochromes.
A helpful conceptual analogy is digital imaging: just as a photograph requires sufficient pixels to resolve distinct objects, accurate spectral separation requires sufficient detector sampling to resolve distinct emission patterns. Modern spectral systems employ detector arrays that substantially exceed the number of fluorochromes used in a panel. Although differences in detector technology (such as detector array number or configuration, or detector types) exist between spectral systems and manufacturers, this redundancy improves robustness, reduces noise, and stabilizes performance, particularly in complex biological samples. Unmixing then mathematically separates overlapping spectral signals by assigning measured photons to their most likely fluorophore and minimizing spillover. While both compensation and unmixing aim to correct for spectral overlap, unmixing is inherently multivariate and leverages information from the entire emission spectrum rather than relying on pairwise channel corrections. As a result, SFC can distinguish fluorochromes with similar peak emissions but distinct off-peak characteristics, expanding fluorochrome choice without changing downstream gating or interpretive logic.
What Can Change with Spectral Flow Cytometry in Clinical Practice?
Reduced Redundancy Through Consolidation into a Single Tube
In CFC workflows, immunophenotyping panels usually consist of multiple tubes, each containing overlapping "backbone markers" such as CD34, HLA-DR, CD38, or CD45 to allow population identification and comparison across tubes.7–9 While effective, this approach requires substantial amounts of sample cells, reagents, and hands-on/handling time (for example through pipetting or handling of multiple tubes), and the interpretation or identification of populations and immunophenotypes across tubes can be challenging. By its very nature, SFC reduces the need for redundancy by consolidating lineage, maturation, and aberrancy markers into a single tube, eliminating cross-tube normalization while retaining familiar markers and patterns for interpretive consistency. As a result, the number of tubes and reagents required per test can be decreased, which may translate into savings for laboratories by lowering costs of reagents. Likewise, it may decrease medical scientist time spent on sample staining and the number of tubes a medical scientist needs to handle per sample, reducing errors related to sample or reagent swapping.
Improvements in Data Quality and Interpretive Clarity
By reducing ambiguity caused by spillover, SFC has several implications for data quality: First, it paves the way for higher-parameter and more complex panels, as evidenced by the increasing number of high-parameter optimized spectral cytometry panels.10 In the clinical setting, existing ("legacy") immunophenotyping panels can be expanded readily with additional markers of clinical relevance or interest, such as therapeutic targets or biomarkers.6,11 Expanded marker capacity allows for more comprehensive immunophenotypic assessment and may also help resolve challenging differentials such as marrow regeneration, clonal cytopenia, or small atypical populations.6 SFC also enhances rare-event detection and interpretation by enabling finer discrimination of low-frequency aberrant phenotypes, particularly within dense immunophenotypic neighborhoods. Important for hematopathology, spectral systems can specifically account for cellular autofluorescence as an independent parameter. This capability is particularly beneficial in bone marrow or lymph node specimens, where autofluorescence from monocytes, myeloid cells, or stromal components can obscure markers or patterns in conventional approaches.11,12
Clinical Applications of Spectral Flow Cytometry
While already widely used in research settings, SFC is increasingly adopted in clinical contexts where multiplexing demands and interpretive complexity exceed the practical limits of conventional approaches. In this setting, consolidated, high-parameter panels facilitate detection of rare or subtle abnormalities, cellular function states, and immune reconstitution patterns that usually require multiple assays or sequential testing strategies, or are poorly resolved in CFC.6,11,12 In acute leukemia immunophenotyping, spectral panels have been validated for acute myeloid leukemia13–16 and more recently B-cell acute lymphoblastic leukemia.17 They have been shown to overcome certain signal/noise limitations, which may improve analytical sensitivity for minimal residual disease (MRD) monitoring. Likewise, the expanded immune-cell characterization provided by SFC allows for better diagnostic resolution in immune-modulated conditions such as primary immunodeficiencies, autoimmune diseases, and transplant immune monitoring. Additionally, SFC allows for improved characterization of the tumor microenvironment, or immune reconstitution, where activation states, exhaustion signatures, maturation delays, and immune-recovery patterns can all be more deeply investigated.2 In solid tumor clinical trials, SFC has proven valuable in investigation of tumor-infiltrating lymphocytes, expanding understanding of the tumor microenvironment.11
Operational and Validation Considerations in Clinical Laboratories – What's the Catch?
From a historical perspective, there is often a 10- to 15-year lag between research innovation and clinical implementation, making this a prime time for the clinical adoption of SFC. However, despite its technical advantages, SFC may not be universally optimal for all laboratories or assays.18 While there is significant potential for operational efficiency related to reagent costs, medical scientist time, and specimen requirements (ie, sample volume or total cell numbers required) once a particular assay is optimized, validated, and clinically deployed, considerable upfront investments are needed. These include substantial cost for spectral instrumentation and reagents, as well as time and resources related to assay development and optimization, assay validation, and training.12,18 Moreover, SFC adds operational complexity as unmixing and correct interpretation depend on rigorously maintained, single-color reference and autofluorescence controls.18 As with CFC assays, regulatory requirements and best practices must be followed19; thus, reagent, assay, and instrument validation and day-to-day usage require meticulous quality management and documentation. Training and user competency are also a major consideration and expand beyond what is currently expected from flow cytometry specialists20; as such, users must master reference control design, unmixing, failure modes, and interpretation of new patterns or populations. Moreover, additional computational support or specialized analysis software is likely to be needed, especially as artificial intelligence-based approaches are increasingly employed in the analysis of high-parameter data.18 Given these challenges, laboratories with existing panels already validated on legacy cytometers, with high-throughput routine and sufficiently sensitive assays with stable workflows, or without capacity for expanded training or software infrastructure may not experience a net benefit relative to cost and complexity. Of note, grassroot initiatives are currently under way, for example within the International Clinical Cytometry Society (ICCS) community, to more broadly support the implementation and adoption of SFC in clinical laboratories, including the harmonization of panels, markers, reagents, analysis and interpretation. Such initiatives also hold the promise of clarifying and streamlining operational and educational considerations and requirements, ultimately enabling clinical laboratories to make an informed decision whether to invest in this technology.
Conclusion
SFC significantly enhances immunophenotypic analysis with the simultaneous analysis of more antigens in a single tube through the capture of the entire emission spectrum for each fluorophore. SFC may translate to benefits in clinical applications such as MRD, transplant, and diagnostic resolution in immune-modulated conditions. While sample requirements and preparation remain the same, SFC can offer significant productivity and data quality gains for clinical flow laboratories with high volumes or demands for multiplex immunophenotyping, marker complexity, or deep profiling in limited sample volumes. However, the decision to transition from CFC to SFC should be grounded in volume and interpretation needs, laboratory-specific workflows, validation complexity, budget cycles, and training capacity, all of which must be addressed within existing regulatory frameworks. Ultimately, although CFC has reached the limit of its technical capacity and SFC allows for expansion into new heights of data acquisition and analysis, CFC will likely remain a "workhorse" in most clinical laboratories but is likely to be complemented by spectral instrumentation in the future, especially as the availability of clinical instruments increases.
References
- Robinson, JP. Spectral flow cytometry-quo vadimus? Cytometry A. 2019;95:823-824.
- Robinson, JP. Flow cytometry: past and future. Biotechniques. 2022;72:159-169.
- Nolan JP. The evolution of spectral flow cytometry. Cytometry A. 2022;101:812-817.
- Shapiro HM. Practical Flow Cytometry. Wiley; 2003. doi:10.1002/0471722731
- Introduction to Flow. https://www.youtube.com/watch?v=n7UULWuPSsg ICCS YouTube Channel. Published 2025. Accessed April 26, 2026.
- Czechowska K, Bonilla DL, Dankar A, Mead PE, Nash V. Beyond the limits: how Is spectral flow cytometry reshaping the clinical landscape and what is coming next? Cells. 2025;14:997.
- Cherian S, Wood B, Borowitz MJ. The flow cytometric evaluation of hematopoietic neoplasia. In Henry’s Clinical Diagnosis and Management by Laboratory Methods. Elsevier; 2016.
- Karlon WJ, Dorfman DM, Linden MA. Color Atlas of Flow Cytometry. College of American Pathologists; 2023.
- Lucas F, Cherian S, Linden MA, Tashakori M. Flow cytometry in acute myeloid leukemia (AML): a critical tool for accurate diagnosis, classification, and monitoring. Clin Chem. 2025:hvaf111. doi:10.1093/clinchem/hvaf111
- OMIPs Collection. Wiley Online Library Accessed December 1, 2025. https://onlinelibrary.wiley.com/doi/toc/10.1002/(ISSN)1552-4930.OMIPscollection
- Brestoff JR. Full spectrum flow cytometry in the clinical laboratory. Int J Lab Hematol. 2023;45(suppl 2):44-49.
- McCausland M, Lin YD, Nevers T, Groves C, Decman V. With great power comes great responsibility: high-dimensional spectral flow cytometry to support clinical trials. Bioanalysis. 2021;13:1597-1616.
- Soh KT, Conway A, Liu X, Wallace PK. Development of a 27-color panel for the detection of measurable residual disease in patients diagnosed with acute myeloid leukemia. Cytometry A. 2022;101:970-983.
- Chen M, Fu M, Gong M, et al. Twenty-four-color full spectrum flow cytometry panel for minimal residual disease detection in acute myeloid leukemia. Open Med (Wars). 2023;18:20230745.
- Fokken H, Waclawski J, Kattre N, et al. A 19-color single-tube full spectrum flow cytometry assay for the detection of measurable residual disease in acute myeloid leukemia. Cytometry A. 2024;105:181-195.
- Gao Q, Chan A, Zhang J, et al. 28-color single tube for flow cytometric assessment of myeloid maturation, myeloid neoplasia, and acute myeloid leukemia minimal/measurable residual disease. Cytometry B Clin Cytom. 2025;108:198-211.
- García-Aguilera G, Castillo-Robleda A, Sanz A, Ramírez M. Validation of a spectral flow cytometry single-tube panel for the clinical diagnosis and follow-up of children and adolescents with B-cell acute lymphoblastic leukemia. Cells. 2024;13:1891.
- Woolard S. Implementing spectral flow cytometry in the clinical laboratory: from adoption to validation. ICCS e-Newsletter. Published 2026. Accessed April 21, 2026, cytometry.org
- Clinical and Laboratory Standards Institute (CLSI). Validation of Assays Performed by Flow Cytometry. 1st ed. CLSI guideline H62. CLSI; 2021.
- Greig B, Oldaker T, Warzynski M, Wood B. 2006 Bethesda International Consensus recommendations on the immunophenotypic analysis of hematolymphoid neoplasia by flow cytometry: recommendations for training and education to perform clinical flow cytometry. Cytometry B Clin Cytom. 2027;72(suppl 1):S23-S33.

Fabienne Lucas, MD, PhD, FCAP, is an assistant professor in hematopathology and the codirector of the clinical flow cytometry laboratory at the Department of Laboratory Medicine and Pathology at the University of Washington, Seattle. With a rich background in hemato-oncology, immunology, and flow cytometry, she currently supports the International Clinical Cytometry Society community as Community and Growth Committee chair and active contributor to several working groups and initiatives. She also serves on the CAP Personalized Health Care Committee as vice chair.

Alexa André, MD, is currently a second year anatomic and clinical pathology resident at the University of Washington with plans to pursue a fellowship in hematopathology. She is a member of the CAP Residents Forum as a resident delegate for the University of Washington. Research interests include educational quality improvement and myeloid neoplasms.

Christopher G. Snyder, MD, PhD, is a hematopathology fellow at the University of Washington, Seattle in the Department of Laboratory Medicine and Pathology and is board-certified in clinical pathology. His clinical interests center on integrated hematopathology diagnosis across morphology, immunophenotype, cytogenetics, molecular testing, and clinical context, with a particular focus on flow cytometry. His academic work emphasizes applied artificial intelligence and informatics for laboratory medicine, including decision support, workflow automation, and tools that reduce friction in multimodal data retrieval and correlation. He is preparing for subspecialty board eligibility in hematopathology following fellowship completion.